
This article was first published in MASS Research Review and is a review and breakdown of a recent study. The study reviewed is Learning One’s Genetic Risk Changes Physiology Independent of Actual Genetic Risk. Turnwald et al. (2019)
Key Points
- In two separate experiments, researchers told people they had either the good or bad version of a gene that affects aerobic exercise, or the good or bad version of a gene that affects appetite and satiety.
- The subjects underwent one testing session before being told they had either good or bad genes, and one testing session after they were told they had either good or bad genes.
- For some measures, the people who were told they had bad genes regressed from the first to the second testing sessions; for other measures, the people who were told they had good genes improved from the first to the second testing sessions. This was true for both objective physiological measures and subjective responses.
- These results aren’t too surprising, as prior research has shown that expectancy affects both acute and chronic outcomes.
Consumer genetic testing is really popular right now, and I can understand the appeal. The Human Genome Project just wrapped up 16 years ago, after 13 years of work and nearly 3 billion dollars of investment. Now, you can send a saliva sample to a lab, pay $99, and gain some insight into your own genetics within weeks. Since genes code for all of the proteins that differentiate you from every other human on earth, it makes sense that people would want to get a glimpse into this very fundamental aspect of their physiology now that it’s become so accessible.
However, a little bit of knowledge can be dangerous. And, more to the point, simply learning about your genes may influence your perceptions and your physiology. In the presently reviewed study (1), 223 participants across two studies were told they had either the “good” version or the “bad” version of two genes: CREB1 and FTO. The CREB1 gene influences aerobic exercise performance, and FTO impacts hunger, satiety, and obesity risk. Crucially, the researchers didn’t accurately inform all of the participants about the gene variant they actually had; half of the people with “good” genes were told they had bad genes, and half of the people with “bad” genes were told they had good genes. The subjects in the first study completed an aerobic exercise test before being told what version of the CREB1 gene they had and completed the same test again after being told about their CREB1 gene. The second study followed the same pattern, but the “test” involved consuming a standardized meal, and the gene of interest was the FTO gene. In both studies, beliefs about one’s genes impacted both perceptual and physiological measures. In some cases, people who were told they had the bad version of a gene had worse outcomes in the second test than the first test; in other cases, people who were told they had the good version of a gene performed better in the second test than the first test, regardless of their actual genetics.
Purpose and Research Questions
Purpose
The purpose of this study was to evaluate if being told about one’s genetic risks would influence performance, perceptions, and physiology.
Research Questions
- Would thinking that one had a bad genetic draw for aerobic exercise affect respiration or ventilation?
- Would thinking that one had a bad genetic draw for aerobic exercise affect subjective perceptions during an exercise test?
- Would thinking one had a bad genetic draw for aerobic exercise affect performance during an exercise test?
- Would thinking one had a bad genetic draw for obesity affect physiological markers of hunger and satiety following a standardized meal?
- Would thinking one had a bad genetic draw for obesity affect subjective feelings of hunger and satiety following a standardized meal?
Hypotheses
The authors hypothesized that subjects who were informed that they had a “high risk” phenotype would have worse physiological and perceptual outcomes in both experiments.
Subjects and Methods
Subjects
There were 116 participants in experiment 1 (exercise) and 107 participants in experiment 2 (feeding). They were recruited by being told they were signing up for a yearlong “personalized health” study where they’d learn about the best exercises and diets for themselves, based on their genotype.
Study Overview
Both experiments followed a similar flow: have subjects perform a test with no knowledge of their genetic risk for a particular trait, assess physiological and perceptual outcomes, inform (or misinform) them about their genetic risk, and then have them repeat the same assessment a week after the first test.
For experiment 1, the test was maximal effort running on a treadmill. During exercise, the researchers gathered data on the subjects’ CO2:O2 exchange rate and ventilatory flow rate. The subjects were asked about their level of perceived exertion and how hot they felt every two minutes during the test. The gene being tested for was the CREB1 gene; having the “bad” version of the CREB1 gene is associated with lower aerobic exercise capacity, higher body temperatures during exercise, and smaller increases in aerobic fitness following exercise training.
For experiment 2, the subjects ate a standardized 480-calorie meal, with blood samples before eating and 15 and 40 minutes after eating to assess hormones associated with satiety and hunger (GLP-1 and acyl-ghrelin). The subjects also self-reported their subjective feelings of satiety. The gene being tested for was the FTO gene, which is associated with obesity risk and lower satiety.
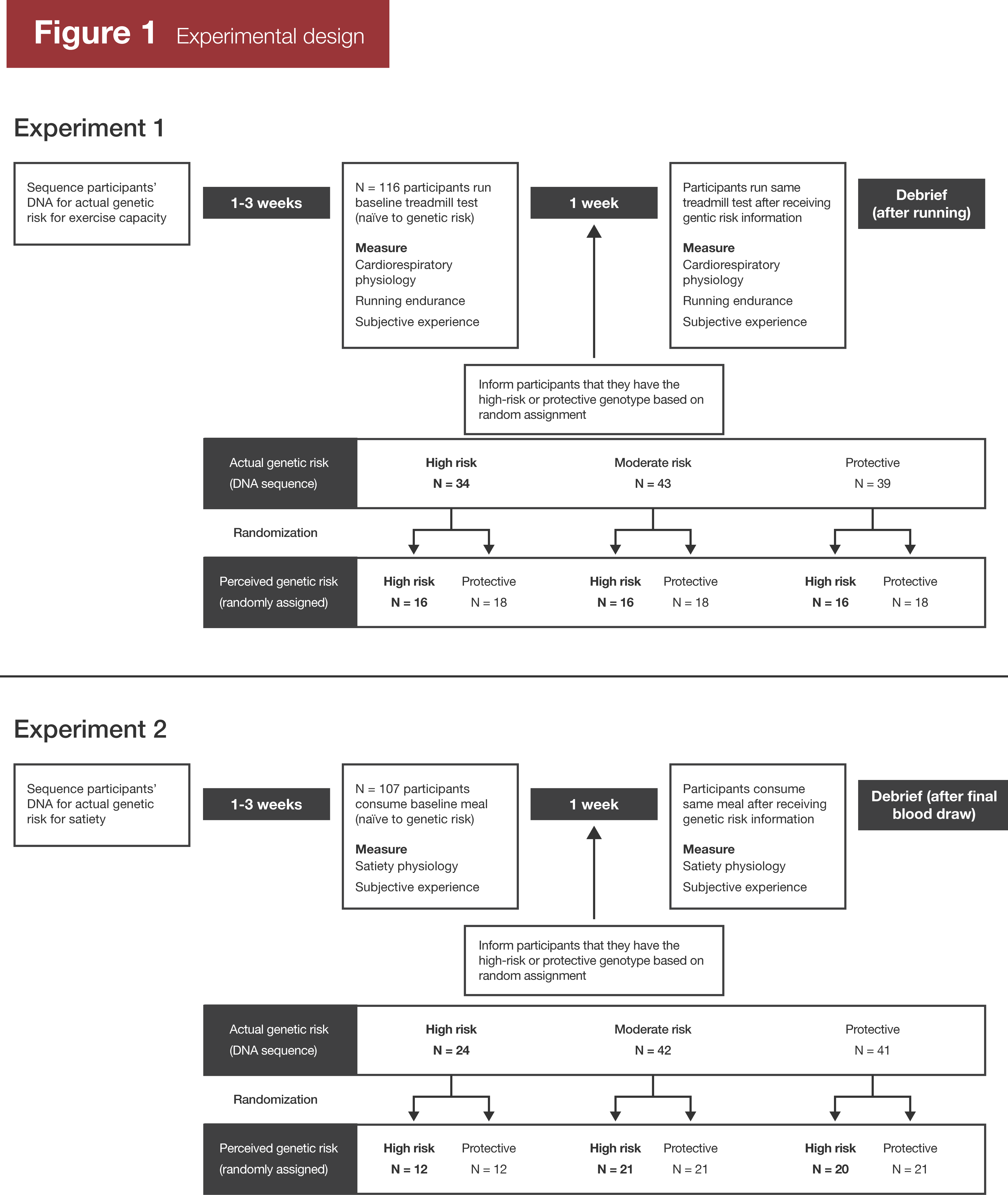
For both experiments, half of the participants were told they had a “good” genotype, and half were told they had a “bad” genotype, regardless of their actual genotype. The authors use the terms “protective” and “high-risk.” Thus, this study was examining the effect of beliefs about one’s genetics, rather than actual genetic differences. Subjects were counterbalanced into each group based on their actual genotype; in other words, if 30 people with a “good” genotype signed up for experiment 1, 15 of them would have been told they had “protective” genes for aerobic exercise, and 15 of them would have been told they had “high-risk” genes for aerobic exercise.
Findings
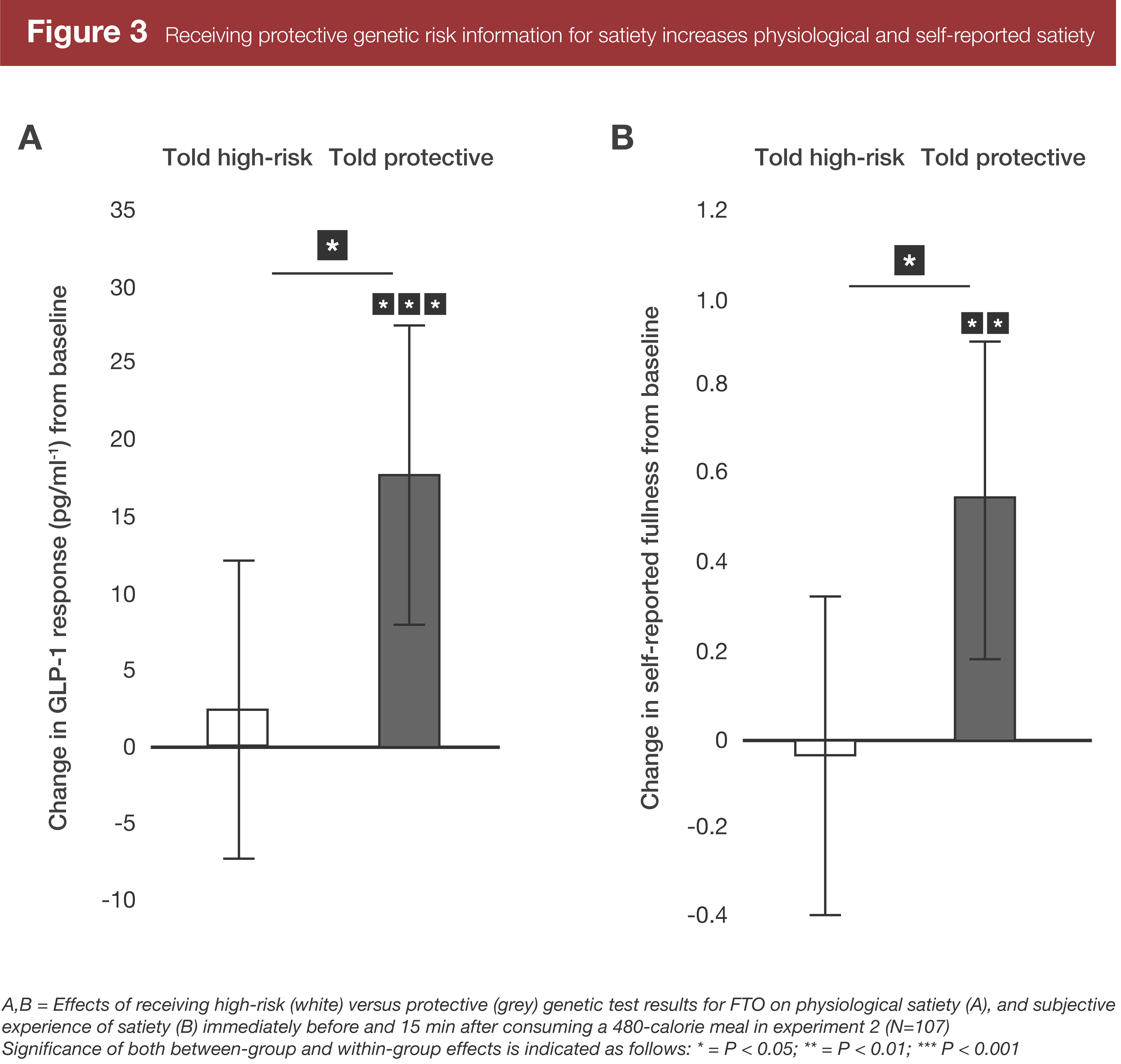
I’ll save you the trouble of trying to parse a wall of statistics since there were a lot of outcomes. Instead, refer to Figures 2 and 3.
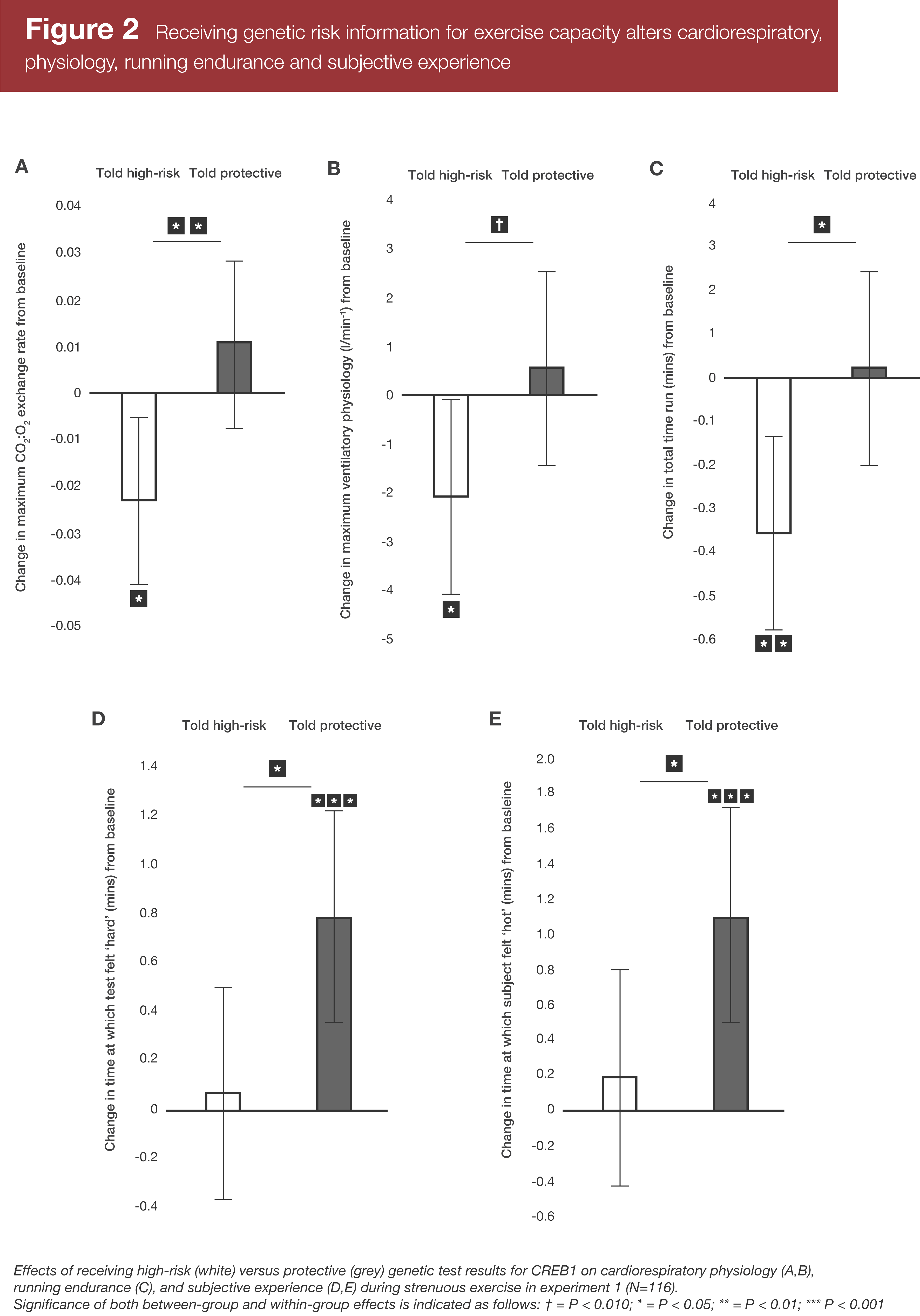
Both experiments found clear differences between conditions. In general, the subjects who were told they had a “high-risk” version of the CREB1 gene had worse outcomes in their second session (after they’d been “informed” about their genotype) for maximal CO2:O2 exchange rate, maximal ventilatory flow rate, and total time spent on the exercise test prior to exhaustion. There were effectively no changes in these measures in the group told they had a “protective” version of the CREB1 gene. On the other hand, the subjects who were told they had a “protective” version of the CREB1 gene had slower increases in perceived exertion during the test, and it took them longer to feel hot during the test in the second session than the first session.
In experiment 2, the group told they had a “high risk” FTO genotype didn’t experience a decrease in a physiological marker of satiety (GLP-1) or in self-reported perceptions of satiety, but the group told they had a “protective” genotype experienced increases in both GLP-1 and perceived satiety. Interestingly, a physiological marker of hunger (acyl-ghrelin) didn’t change significantly within the entire cohort. However, it did significantly change in the individuals who actually had the “good” and “bad” versions of the FTO gene, decreasing in people told they had a “protective” genotype and increasing in people told they had a “high-risk” genotype.
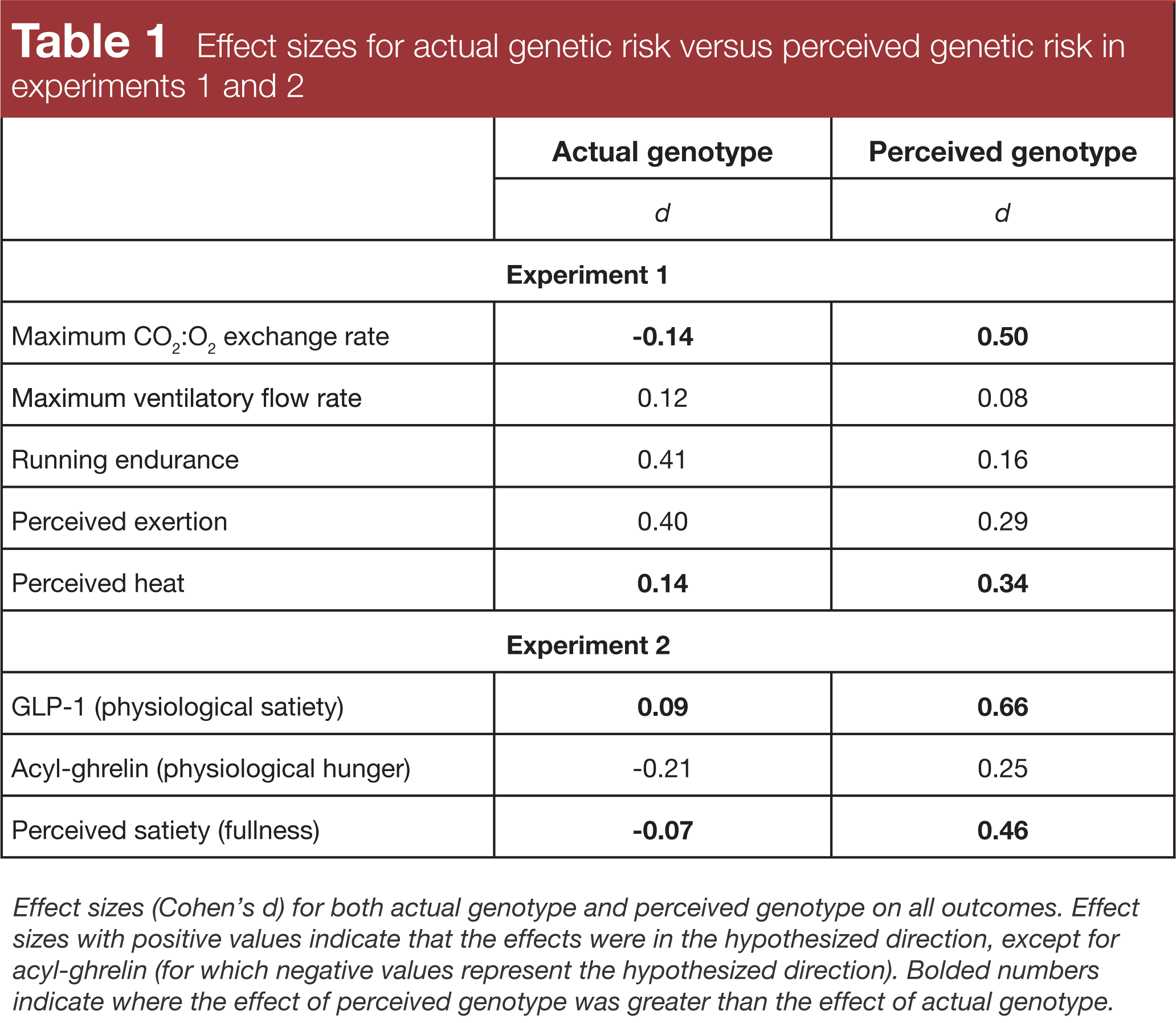
Strikingly, in both experiments, simply thinking you had the good or bad allele variant for these two genes affected several outcomes – both objective and subjective – more than actually having the good or bad allele variant: maximal CO2:O2 exchange rate and perceived heat in experiment 1, and GLP-1 and satiety in experiment 2.
Interpretation
I appreciated this study because it highlights two important issues: the specific issue of gene testing and the general issue of expectancy effects.
Gene testing is getting more affordable and accessible, and I can understand the allure of it: it’s one of the few ways to get a glimpse of “what you’re made of” on a very fundamental level. However, I wonder if it sometimes does more harm than good. As seen in the results of this study, sometimes learning that you have a good genetic endowment for a particular trait can improve outcomes (it’s easier to put more effort into something if you believe you have greater odds of success), but learning you have a bad genetic draw can also lead to worse outcomes. I can’t count the number of people who’ve messaged me, worried because 23andMe told them they had the “bad” version of the ACTN3 gene. They’re afraid they’re just wasting their time in the gym. Does that demotivate them and decrease the effort they put into their training? Would that one gene really make or break their training outcomes (No – one study found that about 50% of elite sprinters have at least one “bad” copy of that gene; 2)? I often think that, at least for the optimist, ignorance can be bliss. If you can convince yourself you have a good genetic draw for your chosen undertaking, and you can resist the urge to find out whether that belief is correct, you’re probably better off than you would be if you got genetic testing and found out you had a bad genetic draw.
It’s also worth noting that current consumer-grade genetic testing doesn’t tell you nearly as much as it would like you to believe. Some single genes have a huge phenotypic impact – mutations in a single gene can cause sickle cell anemia or Huntington’s disease – but most do relatively little in isolation. For example: FTO, the gene tested in experiment 2 of this study, is the gene most associated with obesity risk that we’re currently aware of. How much of an independent effect does the “bad” version of this allele have? About 0.3 BMI points, which corresponds to about 1kg of scale weight (3). It also doesn’t negatively affect the efficacy of weight loss interventions (4). The reason for this is simple: Most traits we care about are massively polygenetic. Lots of genes play a role, so knowing about a mere handful of genes (and generally no more than one or two for each trait) from a consumer-grade genetic testing service doesn’t really tell you much. For example, as of 2011, there were at least 22 genes known to contribute to the “strength/power” phenotype (5). Knowing about only ACTN3 still leaves you 95.5% in the dark.
I wrote an article several years ago titled “Unleash Your Inner Superhero.” Looking back on it, the title is corny as hell, but it’s still one of my favorite articles I’ve written. The primary point of it is that expectancy can have real, measurable effects on your physiology. For example, in one study (6), participants all drank a 380-calorie milkshake, but the researchers put different labels on the milkshakes. One of the labels said the milkshake was 620 calories, and the labeling portrayed it as delicious and indulgent. The other label said the milkshake was a scant 140 calories and was a sensible, figure-conscious choice. After drinking the milkshakes, the researchers monitored the participants’ ghrelin levels (higher ghrelin generally means greater hunger) and their feelings of fullness and satiety. The group that thought they drank an indulgent 620-calorie milkshake had steep drops in ghrelin and reported being quite full and satiated, whereas the group thinking they drank the sensible 140-calorie milkshake maintained fairly consistent ghrelin levels and reported being hungrier.
In another study (7), researchers recruited 15 lifters, had them train for seven weeks, and told them that the people who got the best results could be given free steroids. In those seven weeks, the lifters put a combined total of ~22 pounds on their bench, military press, seated press, and squat, on average. Then, six of the participants were selected at random to take part in the “steroid” trial. They were told they were being given 10mg/day of Dianabol. Really, they were taking placebo pills. They trained for another four weeks, thinking they were on drugs. In just four weeks, they put a combined total of ~100 pounds on those same four lifts, meaning their rate of progress probably increased almost eight-fold simply because they thought they were on steroids (and thus expected to make much better progress). I think the findings of the presently reviewed study reinforce this point: Expectancy influences outcomes.
Now, I want to make something very clear: Genetics absolutely matter. You can’t just rely on expectancy to make it to the top of the heap in your chosen pursuits. My point is more that knowing about a handful of allele variants from a consumer genetic testing service doesn’t really tell you much about your athletic propensities, but it does pose a non-negligible risk of screwing you over if you find out you don’t have a perfect genetic draw for your chosen sport and if that knowledge has a negative impact on what you expect from yourself. As I’ve been saying for years now, you don’t truly know how good your genes are until you train for a decade with the expectation that you have good genes.
Next Steps
I’d love to see a simple training study in which the subjects’ expectations are manipulated. For example, it could start with an informational session where the researchers tell the subjects in one group that the training program they’re about to start generally increases strength by 20%, while telling the other group that the training program is simply designed to maintain strength. This message could be reinforced throughout the study by using periodic maxes; people in the first group could be told they’re “on schedule” to gain as much strength as they should or that they’re falling behind, while people in the second group could be told they’re doing a great job maintaining their strength, or that the researchers are surprised if/when they get stronger.
Alternately, this hypothetical study could be set up in a manner similar to the study reviewed in this article, with half of the subjects told they have good genes for strength gains and half the subjects told they have bad genes for strength gains.
Application and Takeaways
It may be risky to have gene testing done. If you find out you have good genes for lifting, that may improve your outcomes, but it may also be self-limiting if you learn you don’t have ideal genes for lifting. Furthermore, consumer genetic testing services don’t test enough genes that are relevant for strength and hypertrophy for the results to be of much use in the first place. For the time being, I think the best approach is to just assume you’re genetically blessed (or to accidentally get your hands on some placebo steroids).
References
- Turnwald BP, Goyer JP, Boles DZ, Silder A, Delp SL, Crum AJ. Learning one’s genetic risk changes physiology independent of actual genetic risk. Nature Human Behavior. 2019; 3:48-56.
- Yang N, MacArthur DG, Gulbin JP, Hahn AG, Beggs AH, Easteal S, North K. ACTN3 genotype is associated with human elite athletic performance. Am J Hum Genet. 2003 Sep;73(3):627-31.
- Qi Q, Kilpeläinen TO, Downer MK, et al. FTO genetic variants, dietary intake and body mass index: insights from 177,330 individuals. Hum Mol Genet. 2014 Dec 20;23(25):6961-72.
- Livingstone KM, Celis-Morales C, Papandonatos GD, et al. FTO genotype and weight loss: systematic review and meta-analysis of 9563 individual participant data from eight randomised controlled trials. BMJ. 2016 Sep 20;354:i4707.
- Hughes DC, Day SH, Ahmetov II, Williams AG. Genetics of muscle strength and power: polygenic profile similarity limits skeletal muscle performance. J Sports Sci. 2011 Oct;29(13):1425-34.
- Crum AJ, Corbin WR, Brownell KD, Salovey P. Mind over milkshakes: mindsets, not just nutrients, determine ghrelin response. Health Psychol. 2011 Jul;30(4):424-9; discussion 430-1.
- Ariel G, Saville W. Anabolic steroids: the physiological effects of placebos. Medicine and Science in Sports. 1972 4(2):124-6.


