

As the old adage goes, you are only as strong as your weakest link, and grip strength can be the limiting factor in performance for many different strength athletes. Whether you are a powerlifter, strongman, weightlifter, Crossfitter, or a recreational lifter who wishes to be all around strong, life is better with a strong grip. In this article we are going to explore the science and practice of grip strength training and forearm muscle development. While I will be referencing strength athletes throughout this article, the same information can be applied to enhancing grip strength for athletes in a variety of other sports such as rock climbing, obstacle course racing, wrestling, Brazilian jiu-jitsu, and archery. For readers who are more concerned with aesthetics over grip strength, this article will also delve into how to increase the size of the forearm musculature and which muscles are most impactful to total forearm size.
Types of Grip
Broadly speaking, I’ll classify gripping exercises into three different primary categories with the recognition that there are other legitimate ways to classify them and that my definitions are not universally used. The most common type is support grip, which is used for a wide variety of strength training exercises such as deadlifts, rows, pullups, and farmer’s walks. Since most individuals who strive to improve grip strength prioritize support grip, I will be discussing this type of grip most often throughout this article.
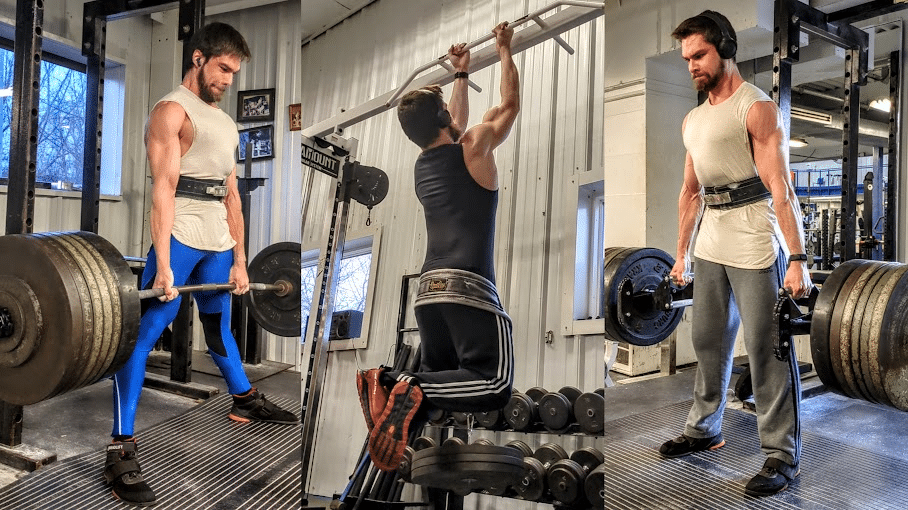
Less frequently utilized is the pinch grip, which as the name suggests, can be trained with plate pinches or pinch blocks. Support grip and pinch grip exercises are both performed with a static intent, but I consider the primary difference between them to be the direction of resistance relative to the hand. If we think of our palm as a laser pointer, this imaginary laser will be directed closer to parallel with the line of resistance during a pinch grip exercise, while it will be directed closer to perpendicular with the line of resistance during a support grip exercise. For instance, during a mixed grip deadlift, resistance is provided by gravitational force acting on the weight in a downward direction, while your palms are facing forward and backward. If we imagine a laser pointing out of the palms, close to a right angle is formed between these lasers and the vector of gravitational force. When holding a weight plate with a pinch grip, the palm is pointed mostly downward close to parallel with the vector from gravity acting on the weight plate. Given this difference in orientation, substantially less load can be used for pinch grip exercises that require you to generate a high amount of friction force in order to maintain finger contact with the implement.


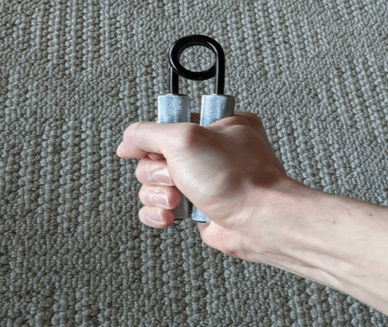
The third type of grip is the crush grip, which is often trained dynamically with hand gripper devices but can also be trained statically by attempting to crush an object like a baseball. In contrast to support grip or pinch grip exercises that typically are loaded via gravitational forces, the resistance for a crush grip exercise is generated internally by the implement. For instance, a torsion spring usually provides the resistance when crushing a hand gripper. In accordance with Newton’s third law of motion, a force that is equal and opposite to your crushing force can serve as the resistance when statically attempting to crush something like a baseball.
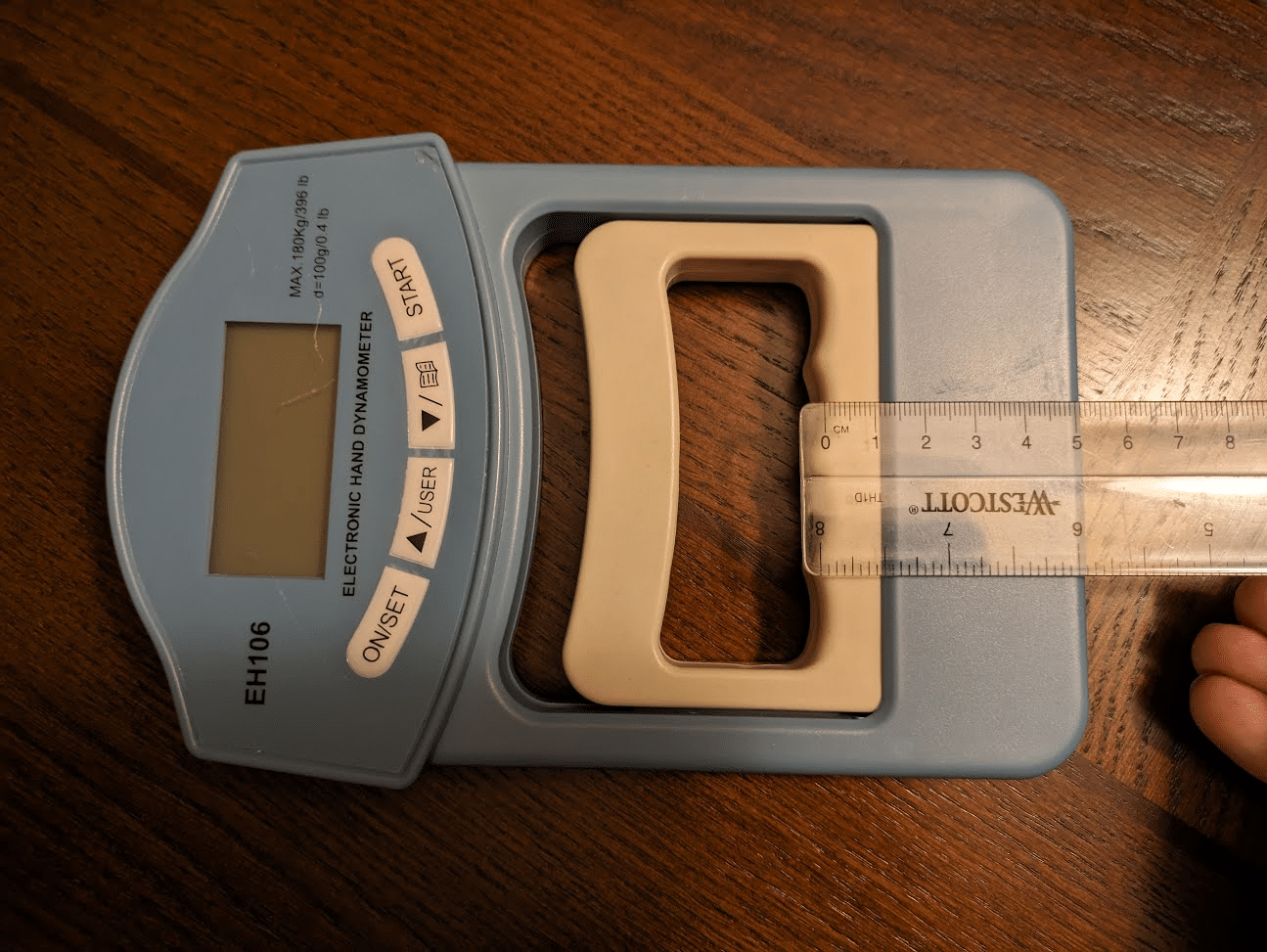
While not involved in most gripping activities, crushing grip is by far the most commonly tested type of grip strength in research due to the accuracy, reliability, and ease of use of grip dynamometers (72,165). In addition to being an outcome value that can be used to track rehab progress in a quantitative manner after a variety of upper extremity or neurological injuries, crush grip strength measured with a grip dynamometer is also a marker of overall health (24,26). Even when controlling for muscle mass, researchers have reported that grip strength is inversely related to all-cause mortality, and it can be an even stronger predictor of cardiovascular mortality than systolic blood pressure (i.e., the top value in a blood pressure measurement) (67,109,110,127,144,146,164,171). Rather than purely being a causal relationship, I suspect that the magnitude of this relationship is influenced by grip strength being positively associated with other variables conducive to health such as full body strength and bone mineral density (115,159,177,209). Other strength metrics such as bench press and leg press 1RMs are also significantly associated with mortality risk, so grip strength does not necessarily have a unique relationship to longevity relative to any other type of strength (71,204). Specifically for elderly women, declining hip flexor strength is also more strongly associated with elevated mortality risk than declining grip strength (213). However, maximal grip strength can be tested on a mass scale more readily than other types of exercise that may require a certain degree of technical proficiency to perform safely (e.g., back squat 1RM) or need expensive specialized equipment (e.g, isokinetic dynamometer). The hydraulic grip dynamometers that are commonly used in clinical settings may cost hundreds of dollars, but a variety of different digital dynamometers can be purchased for about $30 and yield measurements that are reasonably similar to the gold standard (i.e., less than 10% of a difference) (134). In addition to using dynamometers to track whether a block of grip strength training has been productive, some lifters will use these devices as part of a neuromuscular readiness assessment in a similar way to heart rate variability or vertical jump height (76,206). To my knowledge, the potential for an acute grip strength measurement to function as an indicator of systemic fatigue has yet to be studied in lifters.


A foundational principle of exercise science is that the adaptations that occur after a select type of training are specific to the particular demands imposed by that type of training. Consequently, if you want to improve your strength with a particular type of grip, you should be training that specific type of grip. However, this does not mean that maximizing specificity is the key to maximizing results. There is a reason why training for successful powerlifters is not exclusively composed of maxing out in their competition style squat, bench press, and deadlift.
For some individuals, grip strength will not be a limiting factor in performance of competition movements if they consistently perform their sport specific training, but this is not always the case. The volume of training that is required to address a relative grip strength weakness may exceed someone’s recovery capacity if the competition movement is exclusively used for grip training. For instance, if a powerlifter’s deadlift is limited by his grip strength and he already regularly trains deadlifts without straps, simply performing more deadlifts without straps may not be sustainable. Some people can use this approach with success, but others will find that their low backs and hand skin cannot recover from further deadlift volume. To improve deadlift specific grip strength, utilizing a double overhand grip on warm up sets and performing a static hold during the last rep of a work set are two commonly used approaches. Alongside performing rows, vertical pulls, farmer’s walks, suitcase carries, and rack pull holds without straps, these are simple, time-tested methods for improving deadlift grip strength. However, you can use a variety of other training methods to increase long-term grip strength and forearm muscle mass in a manner that is less fatiguing than simply performing more deadlift specific training. To reap the greatest performance transfer to a particular type of grip, keep in mind that these lower specificity forms of training should be used to supplement your sport specific grip training rather than replace it.


Grip Anatomy and Physiology
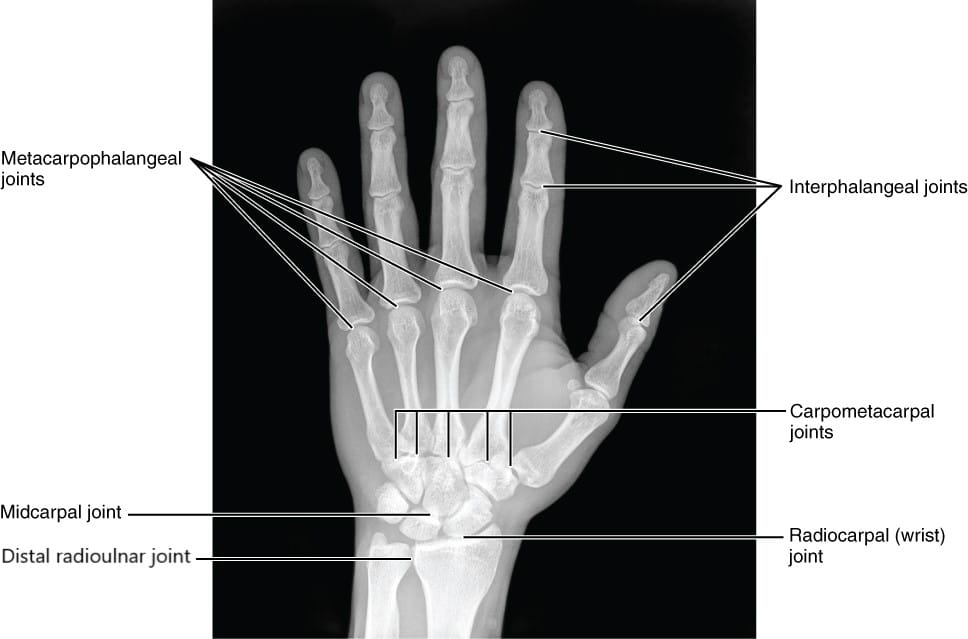
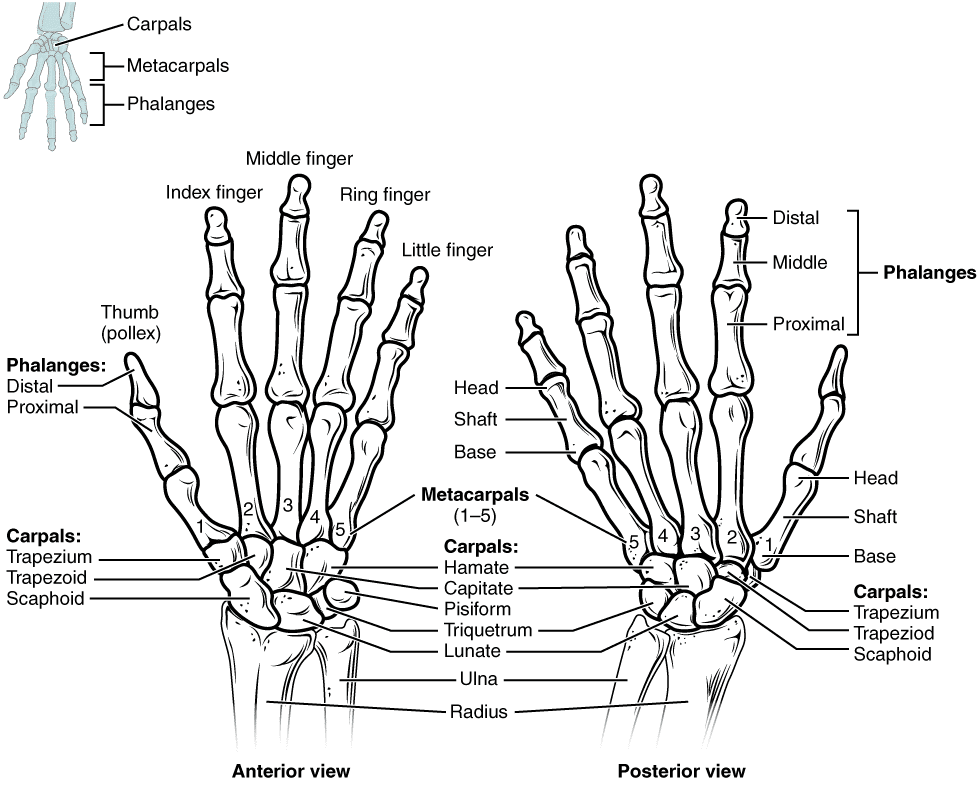
The human hand has 27 bones that are classified into three groups. Most distally (i.e., furthest away from the arm) lie the 14 phalanges that constitute the skeletal structure of the fingers. Together, adjacent phalanges form interphalangeal joints that allow flexion (i.e., bending) and extension (i.e., straightening). With the exception of the thumb, which contains two phalanges and a single interphalangeal joint, each finger has three distinct phalanges and two interphalangeal joints. The one closest to the fingertip is known as the distal interphalangeal joint, while the one closer to the knuckle is known as the proximal interphalangeal joint. The central portion of the skeletal hand is composed of five bones known as the metacarpals, which each interact with a phalange to form a metacarpophalangeal joint that allows flexion, extension, abduction (i.e., spreading apart), and adduction (i.e., coming together).



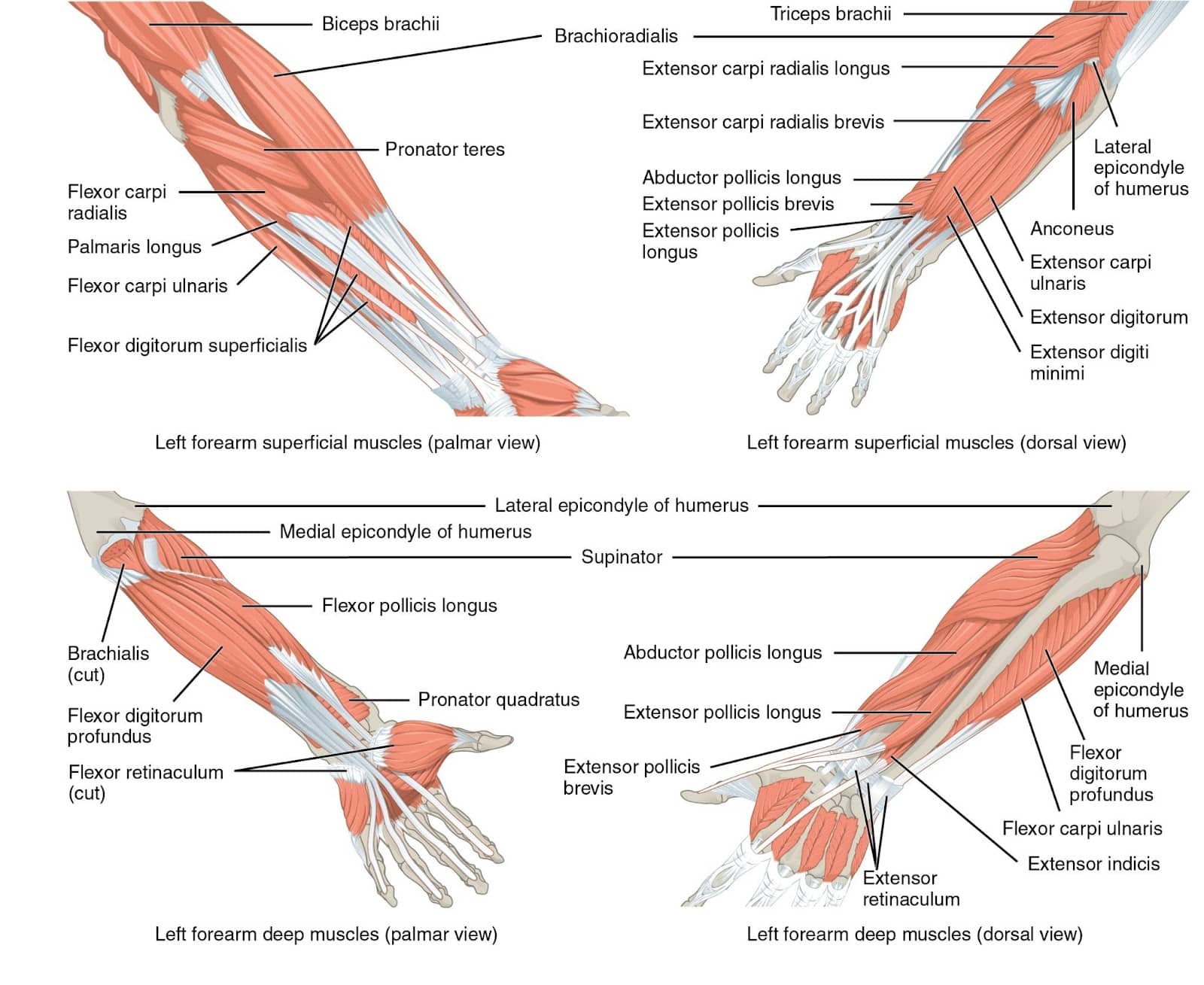
Depending on where they originate, muscles that act on the hand’s joints are classified as intrinsic or extrinsic hand muscles. The muscle bellies of the smaller intrinsic hand muscles are situated within the hand, while those of the extrinsic muscles are situated within the forearm and have tendons that cross the wrist as they course toward the phalanges. Our hands usually contain 19 intrinsic muscles (some people have fewer) that allow us to perform remarkable feats of dexterity only achievable by Homo sapiens (130). Quite relevant to grip strength, the majority of these intrinsic muscles contribute to flexing the metacarpophalangeal joints (11,62,98,211).
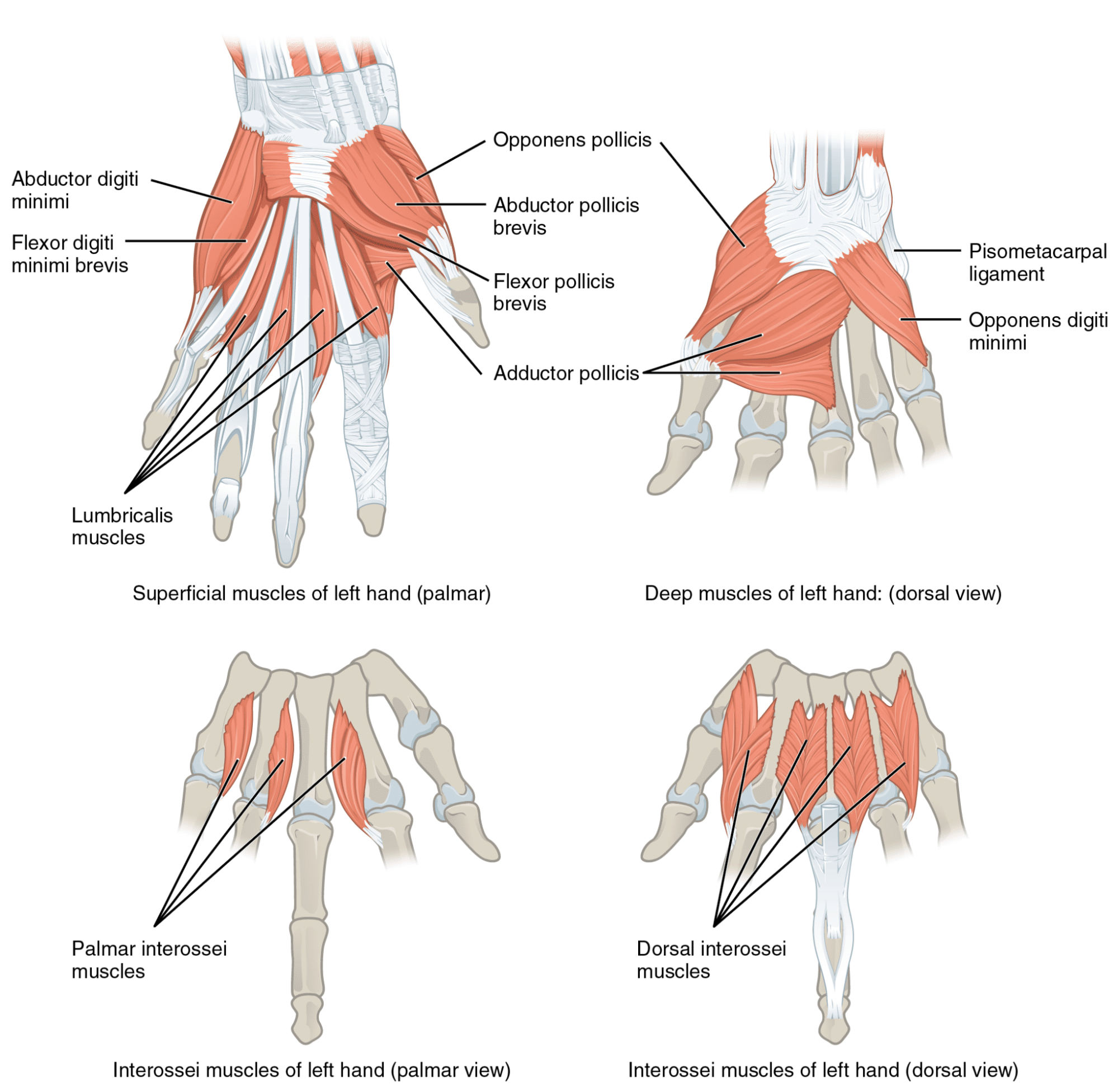
However, much larger extrinsic muscles also cross these joints and are able to generate meaningfully more flexion torque at the metacarpophalangeal joints due to the close relationship between muscle size and force production (31). While I have yet to see the same analysis applied to the thumb, the proportion of total metacarpophalangeal flexion torque that can be produced by the intrinsic muscles varies among the fingers, ranging from 8-28% for the index through little fingers (33,98). For these four fingers, the remainder of metacarpophalangeal flexion torque will be produced by two extrinsic muscles that are indispensable to grip strength performance, namely the flexor digitorum profundus and flexor digitorum superficialis (33,98). Along with the flexor pollicis longus, which flexes the thumb’s joints, these are the only muscles in the body that have the ability to flex the interphalangeal joints. These three extrinsic muscles, located within the anterior (i.e., front) compartment of the forearm, function as wrist flexors along with three other muscles within the same forearm compartment. Due to the extrinsic muscles crossing the wrist and finger joints, wrist position and wrist exercises can meaningfully affect grip strength.
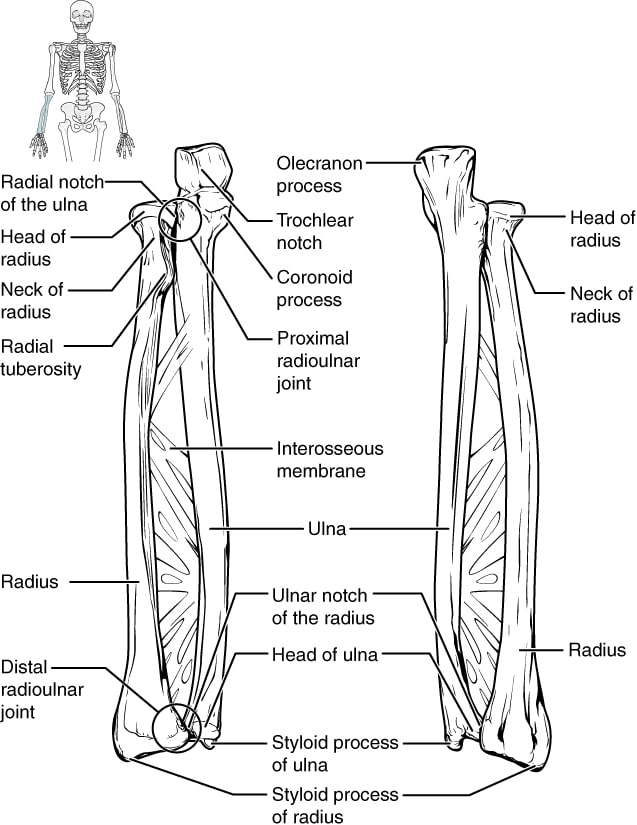
Proximally (closer to the forearm) to the metacarpals lie eight carpal bones that interact with metacarpals to form carpometacarpal joints and each other to form intercarpal joints. In concert with other finger and wrist movements, these hand joints permit variable range of motion, but their details are not particularly relevant to our training (55,131). The three carpal bones that lie closest to the forearm interact with the radius to form the wrist joint (radiocarpal joint), which allows flexion, extension, radial deviation (abduction), and ulnar deviation (adduction). Forearm pronation and supination, which people may sometimes attribute to the wrist joint, occurs as the radius interacts with the ulna at the two radioulnar joints, one of which is right next to the wrist joint while the other lies near the elbow joint.



Determinants of Grip Strength
When tested with a dynamometer, grip strength exhibits an “inverted U curve” relationship with the size of the implement being gripped. An optimal span is present to maximize grip force, and increasing or decreasing the span from that optimum size reduces how much force could be generated (23,54,108,156,168). The average optimal span for producing grip force increases as hand size increases, but most studies find spans close to 55mm (2.2”) to enable the greatest grip force for the typical person (54,64,108,168).
When measuring the individual contributions from the index through little fingers during maximal crush gripping, the middle finger is usually the strongest, followed by the index finger, ring finger, and then the little finger, which is meaningfully weaker than the rest (8,53,107,112,133,161,196). In contrast to the several studies I found that assessed the contributions of the index through little fingers, I was only able to identify a single study that also assessed the contribution of the thumb when maximally gripping with all five fingers (38). Cha et al (2014) attributed 17% of total grip strength to contributions from the thumb, which was less than the contributions from the middle (31%) and index (22%) fingers. Cha et al reported the contributions of the ring and index fingers together (29%), but they stated their findings to still indicate that the little finger contributed the least, which is congruent with the other studies on this topic.
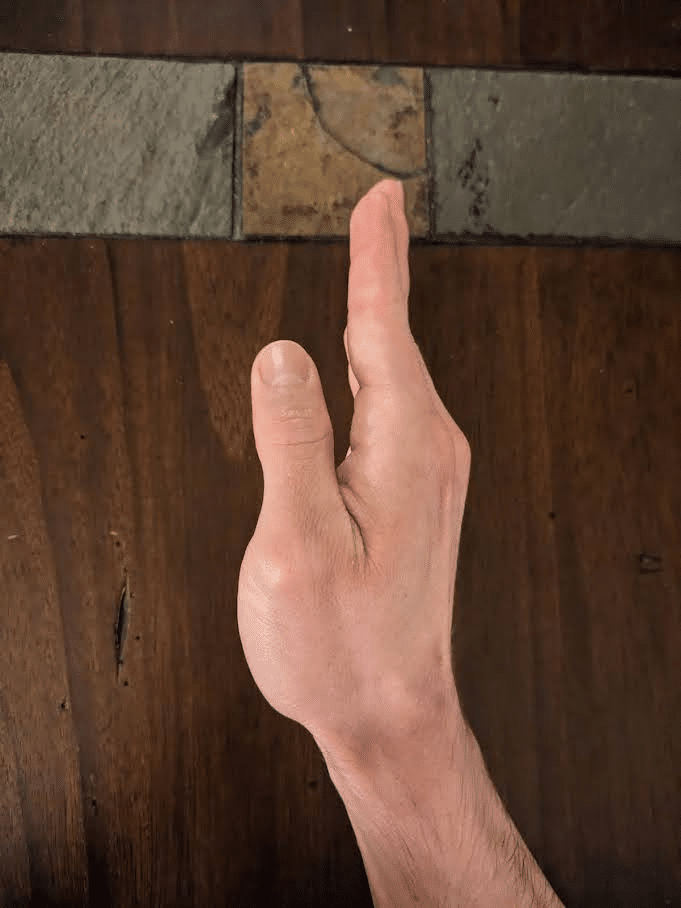
While some pinch grip lifts are an exception that involve extended interphalangeal joints, most types of grip exercises are performed with the interphalangeal joints and metacarpophalangeal joints simultaneously flexed around the implement. Grip failure usually occurs as a lifter is unable to maintain a sufficient degree of flexion at the interphalangeal joints as the resistive force causes them to progressively extend. When gripping an object similar in diameter to a barbell, a lifter may be able to complete a rep if the metacarpophalangeal joints extend and the object drifts toward the fingertips so long as the interphalangeal joints continue to remain flexed.



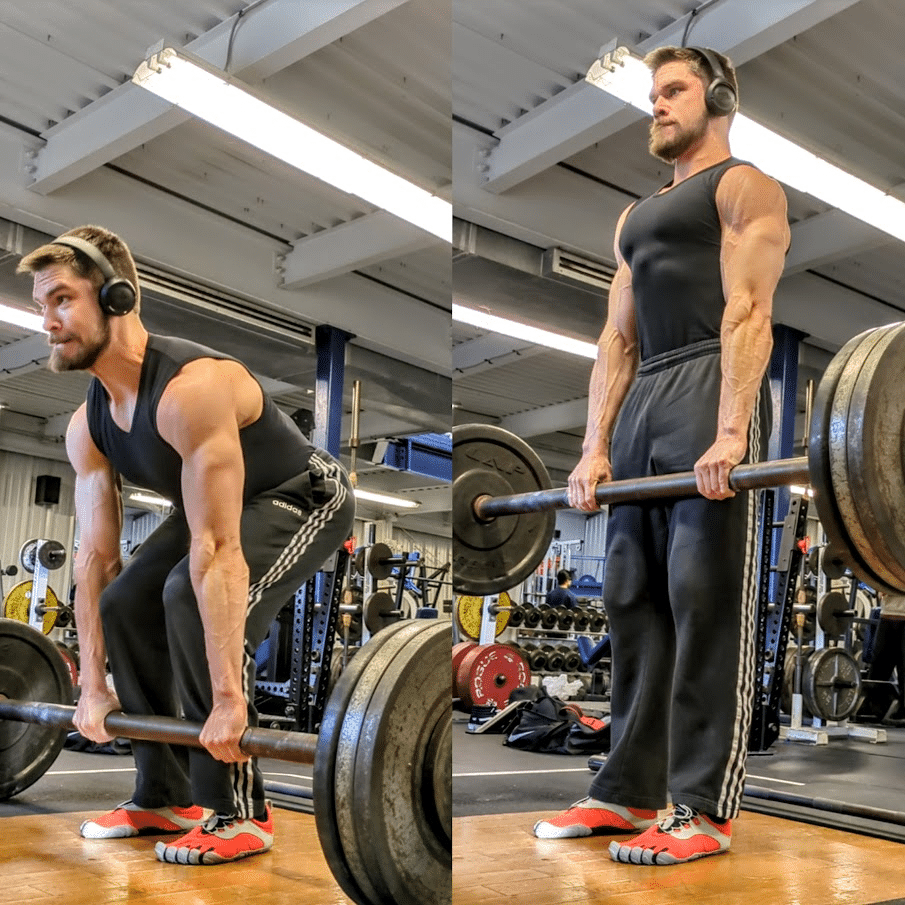
While deadlifting, some lifters will intentionally initiate the pull with this more extended metacarpophalangeal joint position, which some people refer to as a “fingertip grip” position. In contrast, lifters will typically grip a barbell with these joints more tightly flexed as the bar rests closer toward the palm. Compared to using a deeper grip, when beginning a deadlift rep with a “fingertip grip,” the lifter can use a slightly more upright starting position that may be advantageous for someone who has long fingers especially if utilizing a sumo stance. Beyond helping a lifter maintain enough contact with the bar to use a “fingertip grip” successfully, having long fingers (particularly long proximal phalanges) will allow a lifter to start from a more upright position relative to having shorter fingers. Practically this more upright position can make the start of a “fingertip grip” deadlift akin to a very low block pull. Differences among individuals certainly exist, but breaking the floor tends to be the most challenging point in a sumo deadlift more often than a conventional deadlift. Consequently, the “fingertip grip” is more likely to benefit a sumo puller in the same manner that a barbell with greater whip (i.e., deadlift bar) will.

Regardless of which grip is used, nearly every type of gripping activity will rely on someone’s ability to produce flexion torque at the interphalangeal joints and/or metacarpophalangeal joints. Correspondingly, the flexor digitorum superficialis, flexor digitorum profundus, and flexor pollicis longus are the three key grip muscles since they are the only muscles that can flex the interphalangeal joints and metacarpophalangeal joints simultaneously.
Understanding Forearm Muscle Names
Like the hand and foot muscles, the names of the forearm muscles are a mouthful to say, but knowing why they are named this way can make it a lot easier to remember and understand them while not confusing them with other muscles. The “flexor” part at the start of each name communicates that they function to flex the joints they cross. Any muscle with “pollicis” in its name means that it acts on the thumb, while muscles with “digitorum” act on the other four digits. If a muscle has “longus” in its name, it is longer than a muscle performing a similar function that will have “brevis” in its name. For instance, the hand has a flexor pollicis brevis that also flexes the thumb’s carpometacarpal and metacarpophalangeal joint, but it does not act on the wrist or interphalangeal joint because it is shorter than the flexor pollicis longus. “Profundus” is a Latin term for “deep,” so the flexor digitorum profundus lies deeper in the forearm relative to the flexor digitorum superficialis, which lies closer to the surface (i.e., superficially).
Note on Muscle Size Comparisons
Throughout this article, I compare the size of different muscles, and it’s worth noting that most of these measurements are derived from research on cadavers. Naturally, older individuals are more likely to donate their bodies to the advancement of science than younger individuals since the current average global life expectancy is slightly more than 70 years old (which is remarkably greater than the 46 year old global life expectancy in 1950) (74). In the general population, average total muscle mass declines with aging beyond the fifth decade in life (82,111). However, just as fast twitch muscle fibers are more responsive to hypertrophy following resistance training, so too are fast twitch fibers more susceptible to atrophy with aging (111,141,187,203). Consequently, the size of a slow twitch dominant muscle (e.g., soleus) relative to the size of a muscle with a greater percentage of fast twitch fibers (e.g., gastrocnemius) may be greater in cadavers than non-elderly adult lifters (52,215). The general lifting community also trains certain muscle groups much more robustly than others, so average muscle proportions can meaningfully differ between lifters and non-lifters of similar ages. For instance, recreational lifters have exhibited shoulder internal rotation to external rotation strength ratios that are significantly greater than the general population (1,99). While neurological adaptations can contribute to this strength ratio discrepancy, the lifters also most likely have proportionally greater mass of the shoulder internal rotator muscles relative to the external rotators, given the close relationship between muscle size and strength (4). The infraspinatus and teres minor (which are the two primary shoulder external rotators) have been measured to have a combined volume that is about half that of the pec major (a primary shoulder internal rotator) in the general population (77,103). However, lifters generally prioritize training their chests to a greater degree than their rotator cuffs, so their pec majors are likely proportionally larger on average. The overall takeaway from this digression is that the forearm muscle size proportions we cover throughout this article may somewhat differ from those in the lifting community. In the absence of data on muscle proportions of trained individuals, we nonetheless are still using the most pertinent available evidence. While the precise size comparisons will vary among different populations, this variance will not detract from the utility of the practical applications based on this body of evidence.
The Forearm’s Finger Flexor Muscles
Lifters commonly perform wrist curl variations in an effort to improve grip strength, and carryover can indeed be achieved, but not from increasing wrist flexion strength directly. The flexor digitorum superficialis, flexor digitorum profundus, and flexor pollicis longus all have meaningful wrist flexion moment arms, which means they have favorable leverage for generating wrist flexion torque (69,162). Consequently, they can be trained with wrist curls alongside three other muscles in the forearm’s anterior compartment (i.e., flexor carpi radialis, flexor carpi ulnaris, and palmaris longus) (69,162). While all of these forearm muscles have fairly similar wrist flexion moment arms, the flexor digitorum superficialis and flexor digitorum profundus are able to produce the majority of total wrist flexion torque due to their size (69,77,162).
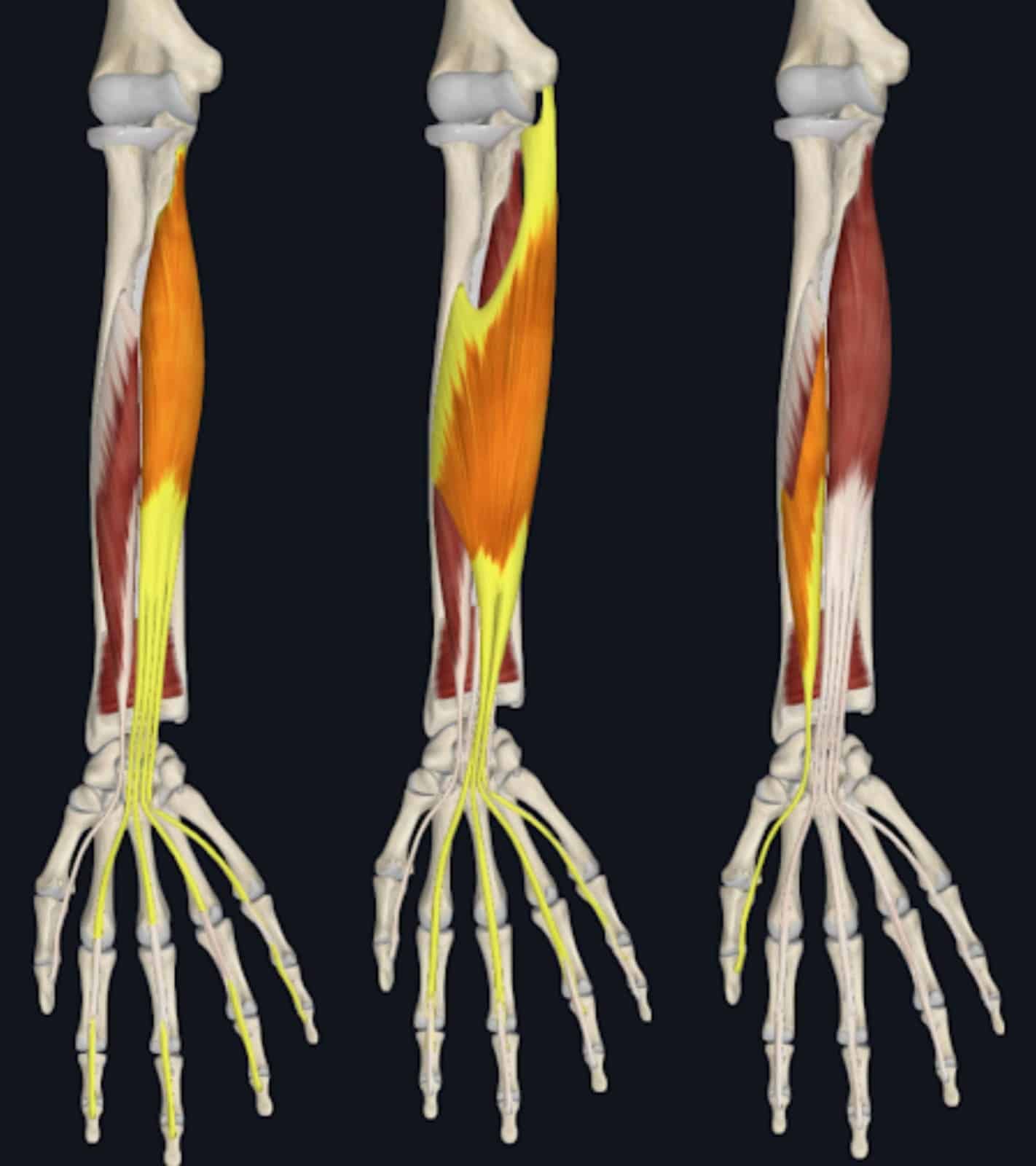
Relative to the flexor pollicis longus, these two muscles generate considerably more force at the wrist and finger joints because their combined cross sectional is about four to seven times greater (depending on the source) (9,69,77). As a result, a given percentage increase in the strength of these two muscles will have a much greater absolute effect on grip strength compared to if the flexor pollicis longus was strengthened by the same percentage. Primarily due to this discrepancy in force production capacity, I consider strengthening the flexor digitorum superficialis and flexor digitorum profundus to be even more important to enhancing grip performance than strengthening the flexor pollicis longus. Furthermore, you may still continue holding onto a bar during a support grip exercise even if your thumb slips off so long as your index through little fingers remain in contact with the implement. With this said, the flexor digitorum superficialis, flexor digitorum profundus, and flexor pollicis longus can all be strengthened simultaneously during a variety of exercises, but I do not deem all three of them to be equally impactful. Training these three muscles through a wrist flexion exercise may transfer to improved grip strength in the same way that training the hamstrings with a knee flexion exercise can transfer to improved hip extension strength (28). Hip hinges and leg curls are not similar movement patterns, but training one of them can increase your strength in the other in large part due to hamstring hypertrophy.
As I previously discussed on Stronger By Science, I do not expect that exclusively training a muscle with isometric exercises that never load the muscle at long lengths is an optimal method of inducing muscle hypertrophy. I have no doubt that performing various pulling exercises and weighted carries can provide a stimulus to the finger flexor muscles to grow up to a certain point given that isometric training certainly can induce hypertrophy (114). However, I am highly skeptical that this style of training by itself could maximize hypertrophy for these muscles in the same way that I doubt that hip flexion exercises (e.g., hanging leg raises) performed without dynamic trunk flexion are an optimal means of growing the rectus abdominis. Muscle size does not necessarily equate to strength, and a lifter can experience significant strength gains due to neural adaptations (154). Nonetheless, in the long-term, the strength potential of a muscle group cannot be fully reached without accruing more contractile tissue. It should come as no surprise that maximal grip strength is strongly positively correlated with forearm muscle size (2,3,83,197). With this in mind, I strongly recommend performing exercises that are well suited to increase the size of the finger flexor muscles if you prioritize increasing grip strength.

To my knowledge, no study has yet to investigate whether training the finger flexor muscles at long peak muscle lengths can induce greater growth than training them at moderate to short muscle lengths. This absence of research applies to most muscle groups in the human body. However, the available body of evidence largely supports that training a muscle in a lengthened position can be a particularly effective method of inducing hypertrophy for a variety of muscle groups (93,94,117,125,210). Unless new evidence emerges indicating that the finger flexor muscles are an exception to this trend, I would program exercises that train them at long lengths when striving to increase their size. Like three of the four hamstring heads, the finger flexor muscles cross more than one joint, so we need to account for the positions of multiple joints when determining the lengths at which they are loaded during an exercise. The finger flexor muscles work at rather short lengths when the wrist and finger joints are simultaneously flexed in the same way that the biarticular (i.e., crossing two joints) hamstrings are fully shortened in a position of knee flexion and hip extension. In this shortened position, the muscles can operate in a state of active insufficiency where force production is submaximal. When the wrist and finger joints are in extended positions, the finger flexor muscles are elongated beyond their resting lengths in the same way that the biarticular hamstrings can be fully stretched when the hip is flexed while the knees are extended.

Wrist Curls and Hand Grippers
During many support grip exercises such as deadlifts and farmer’s walks, the finger flexor muscles will be continually trained at moderately short lengths given the flexed finger joints and neutral wrist position. With a standard wrist curl variation using a tool such as a barbell or dumbbell, these muscles will still be shortened at the finger joints, but they can be lengthened at the wrist as it extends during the eccentric phase of the movement. When accounting for the wrist and finger positions, the finger flexor muscles can be trained at longer peak lengths than most support grip exercises, but they still will not be loaded beyond moderate lengths due to the flexed finger position.


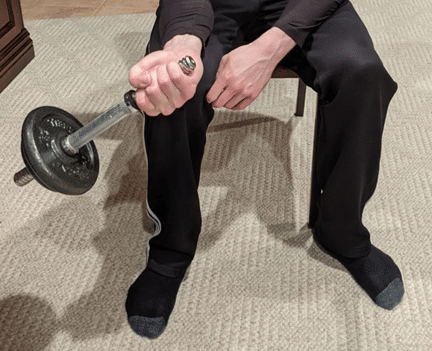
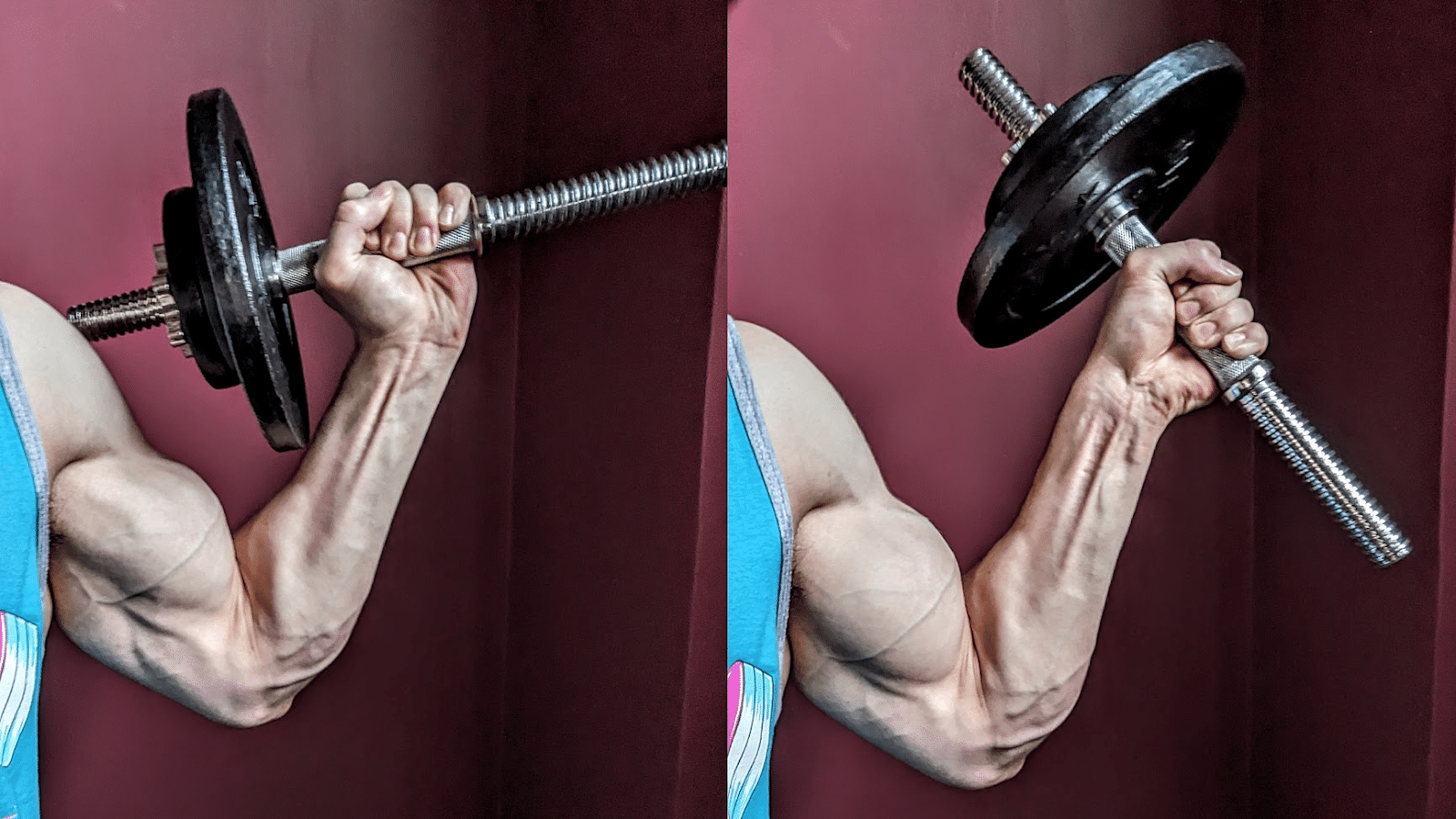
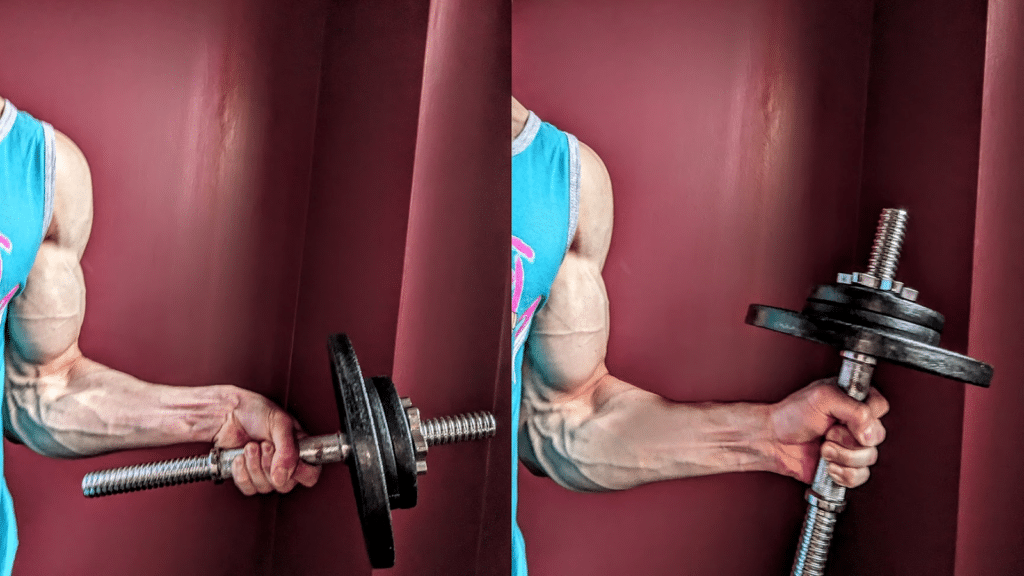
Alternatively, you can perform a wrist curl variation where your fingers dynamically extend (at the metacarpophalangeal joints) during the eccentric phase as the implement rolls toward your fingertips and you extend your wrist, allowing you to train the finger flexor muscles at longer lengths. To maintain control of the weight, you would then flex your fingers around the implement during the concentric phase as you flex your wrist. Doing so will allow you to train the wrist flexion and metacarpophalangeal joint flexion functions of the flexor digitorum superficialis and flexor digitorum profundus simultaneously in a dynamic manner. The addition of metacarpophalangeal joint flexion will also allow you to train the intrinsic hand muscles that assist the larger forearm muscles in performing this function during gripping activities. With this modified wrist curl technique, you need to make sure that the barbell/dumbbell does not roll too far toward your fingertips to the extent that the weight slides out of your hands. Compared to the standard wrist curl technique, you will require less load with this variation to achieve the same difficulty because the lever arm of the resistance acting on the wrist joint increases as the implement rolls toward your fingertips.
To amplify the stimulus per set provided to the flexor digitorum superficialis, flexor digitorum profundus, and intrinsic hand muscles, I recommend that you perform pure finger curl reps once you can no longer perform wrist curl reps due to fatigue. Because the lever arm of the weight acting on the metacarpophalangeal joints is shorter than the lever arm acting on the wrist, ending a set with these finger flexion reps essentially acts as a mechanical drop set. This technique is similar to what I recommend for rowing variations to maximize the stimulus provided to the rhomboids and traps, where you can perform pure scapular retraction reps directly after you can no longer perform any more rowing reps.
Beyond the potential to induce greater hypertrophy, performing wrist curl variations that stretch the flexor digitorum muscles may provide additional mobility benefits for lifters who wish to improve their front rack positioning. When cleaning and front squatting, lifters require a meaningful amount of wrist extension range of motion with extended metacarpophalangeal joints to achieve a stable clean grip front rack. To do so requires a sufficient degree of flexibility in the flexor digitorum muscles that may be lacking for some lifters. While static stretching certainly can be used to increase flexibility, loading muscles in fully lengthened positions via resistance training can yield comparable flexibility improvements (132,183).

By using a hand gripper, you also have the ability to train the finger flexion function of the flexor digitorum muscles in a dynamic manner at longer lengths than could otherwise be achieved with most support grip exercises. With a hand gripper, you can maintain an extended wrist position that allows you to load these muscles at moderate lengths while simultaneously training the smaller intrinsic hand muscles that flex the carpometacarpal joints.

If I could only perform a few sets per week of a single accessory exercise to improve my support grip strength for the deadlift over a mesocycle, hand grippers or wrist curls would not be my top choices. In the short-term, I’d expect a low volume of more specific exercises (e.g., heavy barbell holds) to be most efficient in inducing the desired neural adaptations that can manifest more rapidly than hypertrophy (14,60). Nonetheless, lower specificity exercise can be valuable due to the ease into which they can be added into a program and dynamically train finger flexor muscles at favorable lengths while imparting minimal systemic fatigue. You can train with hand grippers in a host of different environments where any other type of grip training is not feasible, enabling you to accrue greater training volumes without further time commitments in the gym. While not as convenient as grippers, wrist curls can readily be performed during the rest intervals of other exercises you already train that do not tax your grip. Alternatively, you can perform wrist curls at home while watching TV if you have a pair of light dumbbells because they do not require much weight to be challenging to the working muscles. Over time, the hypertrophy that can result from this method of training can make a difference in your long-term grip strength potential. With this said, I still recommend including some heavy training with the precise type of grip you prioritize improving to induce neural adaptations specific to that grip.
Fat Grip and Thick Bar Training
Along with hand grippers and wrist rollers, fat grip attachments that can be added to barbells, dumbbells, or pull-up bars are some of the most popular grip training tools. To my knowledge, fat grip attachments initially became more widely utilized when the aptly named Fat Gripz became commercially available in 2009 with a diameter of 2.25” (57.15mm), doubling the typical barbell diameter of 1.1” (28mm). Today, fat grip attachments come in a variety of sizes, with diameters usually ranging from 1.75” (44.45mm) to 2.75” (69.85mm). When fat grip attachments are added to barbell exercises, their utility is quite similar to an axle bar, which often has a 2.0” (50.8mm) diameter and is used in strongman events such as the axle bar clean and press. While generally inexpensive compared to other specialty bars, most commercial gyms and home gyms lack axle bars, and they are still more costly than fat grip attachments without the same portability.

One of the primary advantages of fat grip attachments is that they can be added to exercises you already perform that use a support grip but are not particularly challenging to your grip strength by the time you finish the set due to fatigue in other muscle groups. For instance, when I perform dumbbell rows with a strict technique, my grip is not meaningfully fatigued by the time I finish the set due to back muscle fatigue. However, when I add fat grip attachments, my grip strength is noticeably challenged by the time I finish the set due to back muscle fatigue. If I wish to further amplify the grip training stimulus per set, I can simply perform a static hold until my grip strength fails after completing the rows. Doing so requires little extra time because my grip muscles are already meaningfully fatigued from the fat grip rows. To ensure that I am not compromising the stimulus provided to the back muscles, I select an exercise variation and type of fat grip that allows me to perform a similar number of reps with the fat grips as I would be able to do without the fat grips. Doing so allows me to train grip strength more effectively without training other muscle groups less effectively, therefore increasing training efficiency. Assuming you have other training goals in addition to enhancing grip strength, I would recommend that you be judicious in which exercises you decide to add fat grips in order to not neglect other muscles.
At least two studies (neither of which utilized chalk) have investigated how 1RMs for common exercises that use a support grip may be affected by using fat grip attachments or axle bars compared to a standard barbell. Krings et al (2021) assessed recreationally active men as they performed 1RMs with a double overhand grip for the deadlift, bent over row, upright row, and biceps curl using a standard barbell with or without 2.2” (5.6cm) diameter fat grip attachments (102). They also tested how many bodyweight pull-ups could be completed in one set as a grip endurance metric and reported that their participants completed an average of 11 reps without the fat grips but only 3 reps with the fat grips. When using the fat grips, the mean 1RMs of the deadlift, bent-over row, upright row, and biceps curl were respectively 41%, 30%, 24%, and 5% lower relative to using the barbell by itself.
Krings et al additionally provided some data on how fat grips may influence muscle activation by measuring EMG activation for eight muscles during the aforementioned exercises. Multiple forearm muscles (i.e., flexor carpi radialis, flexor carpi ulnaris, extensor carpi ulnaris, and the extensor carpi radialis muscles) were assessed alongside the triceps, biceps, trapezius, and lateral head of the deltoid. For the biceps curl and upright row, EMG activity did not significantly differ for any muscle when fat grips were present or absent. However, significant differences in certain muscles were present in different EMG outcomes for the other three exercises depending on whether fat grips were used. For instance, peak EMG activity of the biceps was lower when fat grips were applied to rows and pullups, while mean EMG activity of the extensor carpi ulnaris was greater under those conditions. Without delving too deeply into the nuances of the various EMG findings, the main takeaway is that fat grips can pose a trade off in which increased activity of one muscle may be accompanied by reduced activity of another muscles during certain exercises.
Ratamess et al (2007) also tested the 1RMs of resistance trained men as they performed those four exercises in addition to the bench press and overhead press with barbells having a 1” (2.5cm), 2” (5.8cm), or 3” (7.6cm) diameter (163). For the two presses, the 1RMs with the three different bars were similar, and the 1RMs for the biceps curl and upright row were also similar with the 1” and 2” bars. Unsurprisingly, the greatest difference occurred during the deadlift where 1RMs were 28% and 55% lower when respectively using 2” and 3” bars compared to the 1” bar. As was the case for Krings et al, the bent-over row was the second most affected lift, having 1RMs that were 9% and 33% lower when respectively using 2” and 3” bars compared to the 1” bar. When using the 3” bar, the 1RMs for the biceps curl and upright row were also 18% and 26% lower respectively compared to with the 1” bar.
The impact that thicker implements can have on the load that can be utilized for any particular exercise will certainly vary among individuals and be influenced by someone’s relative strengths, anthropometry, and technique. In general, lifters who have large hands and strong finger flexor muscles relative to other muscle groups will tend to be able to perform a greater variety of exercises with thick bars without compromising how much load they can use (163). Using a strict technique that minimizes momentum and contributions from muscles that you do not prioritize strengthening with a given exercise will also increase the breadth of exercise variations for which you can use fat grips without worsening the stimulus provided to an exercise’s prime movers. For instance, if I perform a bent-over barbell row where I control the eccentric phase, have a brief pause at the top and bottom of each rep, and keep my knees and hips in a static position for the whole set, I can add fat grips without sacrificing weight or reps. However, if I perform a “cheat row” where I dynamically use leg and hip drive to move the weight up each rep in an explosive manner, using fat grips or an axle bar will considerably limit how much load I can use and make it a mediocre back exercise.
If you are an experienced lifter, you may be able to subjectively assess how well an exercise targeted certain muscles with or without fat grips. Sensations can be difficult to communicate through words and may not be particularly precise, but it can be very apparent to a trained lifter when a muscle group is acutely targeted by an exercise. Experiencing a burning sensation and a “pump” due to metabolite and fluid accumulation from moderately high-rep sets or a pronounced feeling of tension in the working muscles during lower-rep sets can indicate which muscle groups a particular exercise may be training effectively. Like localized muscular soreness that may manifest after training, these sensations can be useful proxies to better gauge how likely an exercise may be providing a stimulus of a sufficient magnitude to induce adaptation in different muscles. These proxies certainly have their limitations and should be used in concert with other assessments when guiding programming decisions, but I recommend being aware of them when determining which exercises to add fat grips. If you experience a notable burning sensation in your forearm muscles when performing a 20-rep set of rows with fat grips but don’t feel much in your back muscles in contrast to when you row without fat grips, the fat grips may likely be detracting from your back training. However, if you feel similar sensations in your back muscles while rowing with or without the fat grips, this tradeoff between back and grip training is less likely to be present. When making these qualitative observations along with quantifying the number of reps you can perform with a given weight with or without fat grips, you should be able to determine if fat grips deleteriously affect how well different muscles are targeted during a particular exercise.
Besides being added to exercises you already perform (e.g., strict rows, curls, and shoulder raises) that target muscles other than those involved with gripping, applying fat grips to specific grip exercises provides distinct benefits. One such advantage is that fat grip exercises allow you to train your finger flexor muscles at longer lengths more conducive to stimulating hypertrophy than when using smaller diameter implements. With neutral wrist position support grip exercises such as barbell holds and farmer’s walks, fat grips will still not enable you to train the finger flexor muscles at the same lengths that can be reached during different exercises that load these muscles in an extended wrist position. However, the more extended finger joint angles resulting from the addition of fat grips allows you to train these muscles in more lengthened positions that could otherwise be achieved when performing the same exercises with smaller diameter implements.


Another benefit is that lighter weights will be required to provide a grip strengthening stimulus when using fat grips. After already performing deadlift and squat variations, a lifter whose deadlift is limited by grip strength may opt to perform barbell holds from an above-the-knee rack pull or block pull with the goal of increasing grip strength specifically for the deadlift. While not inherently injurious by any means, loading the lumbar spine with compressive forces is a stressor that imposes a recovery cost. Lifters who are already experiencing high volumes of high magnitude compressing loading from their primary lifts may prefer to minimize further spinal loading from their accessory exercises. When using a standard diameter barbell, a meaningful amount of weight will be required to perform a hold with at least a moderately high intensity. If fat grips are used with these holds, noticeably lighter absolute loads will be needed and the exercise will still be fairly specific to gripping a barbell.
While searching through the literature, I have identified three studies that compared the longitudinal effects of training with or without the 2.25” diameter Fat Gripz. The strength outcomes (e.g., pull-ups, deadlifts) of each of these studies were tested with standard diameter bars. Cummings at al (2018) assessed 10 Division 1 collegiate male golfers as they performed three weekly full-body resistance training sessions for eight weeks (45). In contrast to the control group training without Fat Gripz, which did not experience any improvement, the Fat Gripz group significantly increased drive distance and carry distance over the eight weeks. Relevant to lifters, trap bar deadlift 1RM, max pull-up reps, right hand grip strength, and left hand grip strength were also tested before and after the interventions. With respect to the magnitude of effects, the changes that occurred for these variables did not meaningfully differ between groups to any practical degree. Medina et al (2017) assessed 14 male collegiate lacrosse players who performed three weekly training sessions for five weeks, where each session involved three sets to failure of pull-ups (126). Similar increases in grip strength, max pull-up reps until fatigue, lat pulldown 1RM, and lacrosse shot speed occurred in both the group using Fat Gripz and the group not using Fat Gripz for pull-up training. Additionally, Rogers (2016) assessed 13 female university students who performed two weekly conventional double overhand deadlift sessions for four weeks (166). Each session consisted of 25 reps distributed over 5-6 sets, and participants were permitted to use chalk while training with or without Fat Gripz. After the intervention, the Fat Gripz and control groups increased mean deadlift 5RMs respectively by 29.8% and 39.0%. Peak crush grip strength increased by 11.0% in the control group but only 3.6% in the Fat Gripz group.
When evaluating these three studies together, fat grip training did not yield particularly impressive effects on grip strength compared to conventional training. Without over-generalizing these findings, it is reasonable to assert that the addition of fat grips to any exercise will not necessarily result in superior grip strength training. However, it would be erroneous to conclude that fat grip training cannot be a beneficial component of a larger program that aims to increase grip strength. Each of the three aforementioned studies utilized different populations (none of which were strength sport athletes) and had small sample sizes, which is a limitation extremely common in longitudinal resistance training research. As with countless exercise variations, the potential utility of fat grip training is most likely context dependent, and the three studies compared training with only fat grip exercises to training without any fat grip exercises. This “all or none” decision is reasonable when designing a controlled study, but it does not reflect real world training programs. Further research on this topic is required to draw firmer conclusions, but I would be cautious about relying only on fat grips for grip training just as I would be optimistic about their potential utility when sensibly included in a broader program.
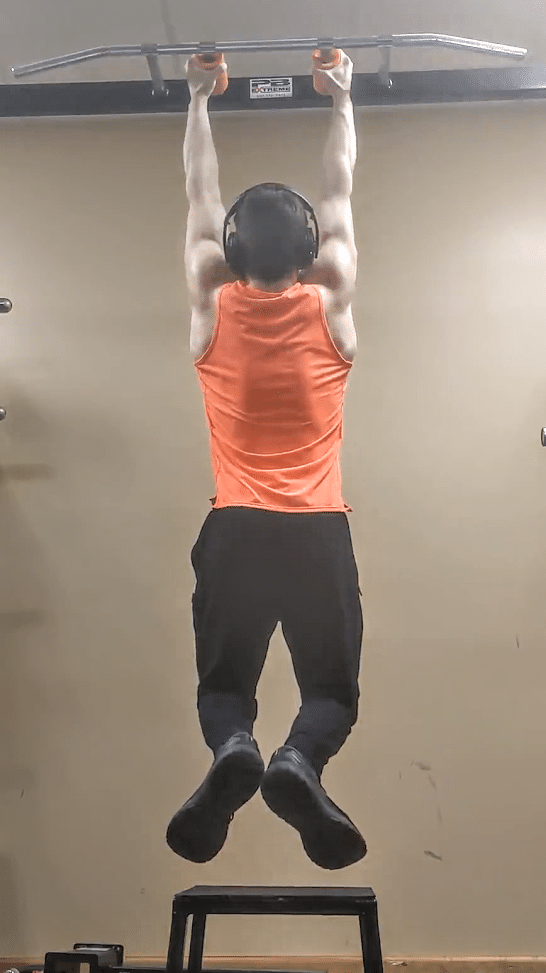
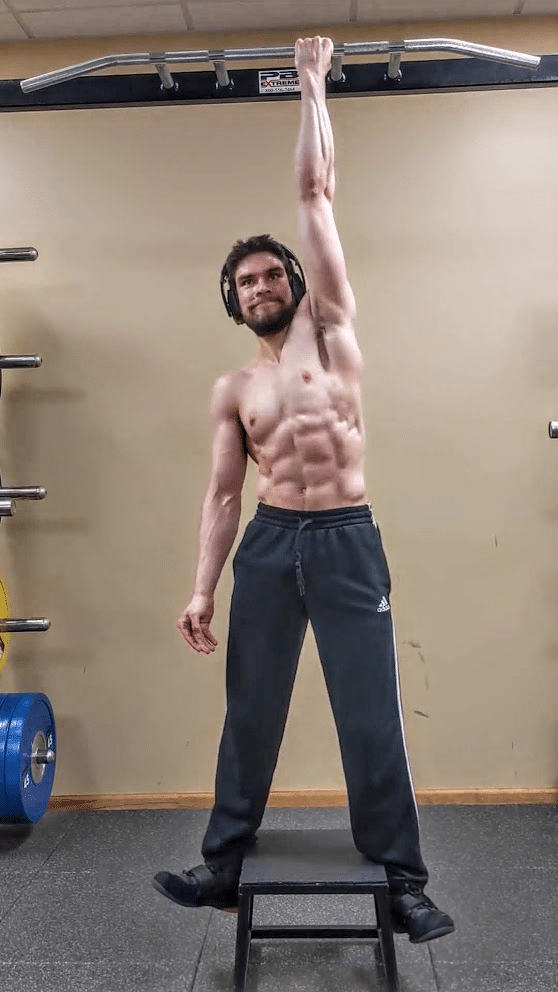
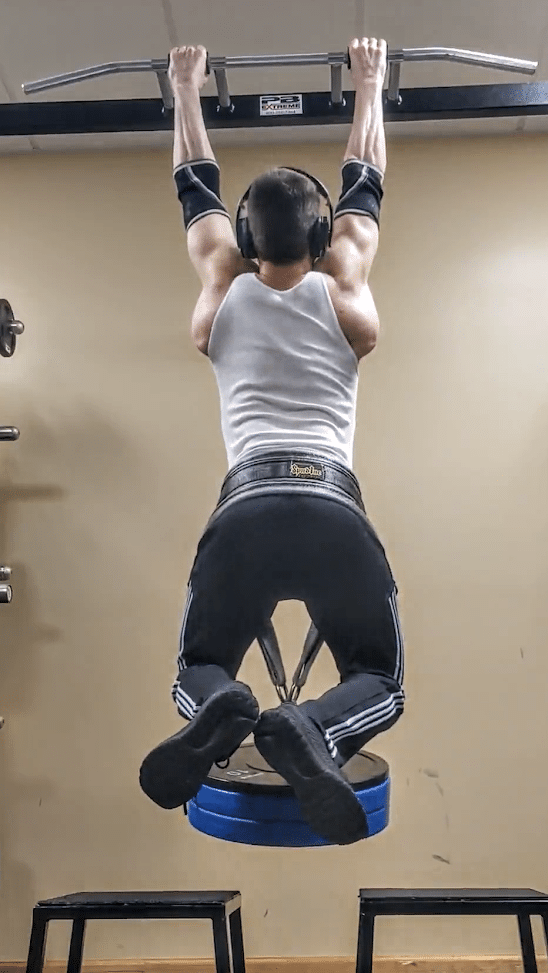
Briefly digressing from fat grip training, the absence of axial compressive loading is a primary reason why dead hangs performed on a pull-up bar are a valuable grip training exercise. Dead hangs allow you to enhance your support grip strength while simultaneously decompressing the spine and training overhead shoulder mobility with a widely available piece of equipment. For individuals with fairly high grip strength to bodyweight ratios who may need to hang bilaterally for a while to challenge their grip strength, unilateral hangs are a simple progression that do not require any extra equipment like a dip/pullup belt to add weights. When performing a unilateral hang, I recommend using your feet or free hand to balance against something such as a rack or doorway to keep your body from unintentionally rotating. With this technique, the intent is not to press down into the object so as to make the exercise easier on your working side (unless you do wish to regress the intensity). Rather, you can use your feet or free hand to merely maintain the starting position you wish to train.
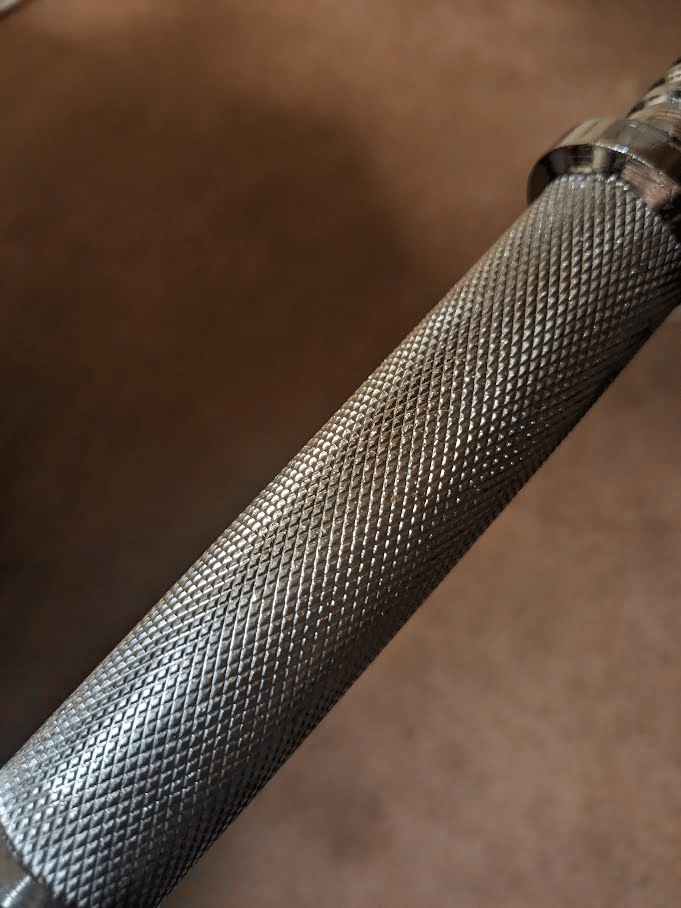
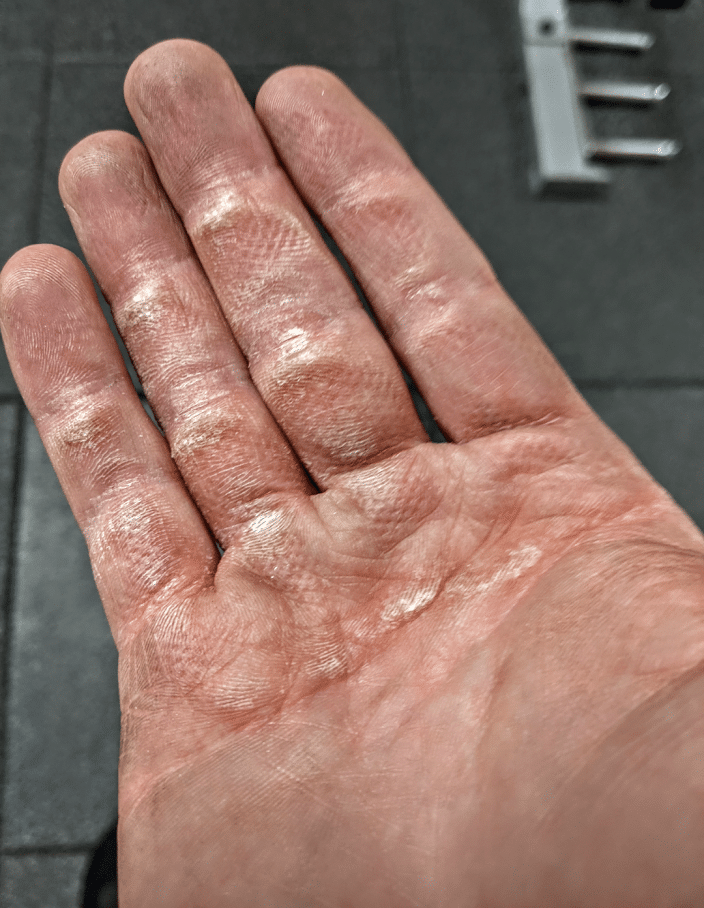
Part of what allows fat grip exercises to challenge your grip strength with lighter loads than standard barbells and dumbbells is the fact that fat grips lack knurling. The knurling found on barbells, dumbbells, and metallic pull-up bars makes gripping the implement considerably easier relative to a smooth surface. Even when using a dynamometer, knurling facilitates significantly greater grip force compared to using a smooth surface (81). With a certain dosage of training with equipment that has pronounced knurling, you will be able to condition your skin and develop calluses that protect your hands. However, your hand skin can only recover from so much grip training with implements that have aggressive knurling before you risk tearing a callus that can interfere with your training and other daily activities throughout the next week. After your hand skin has been sufficiently stressed by training with equipment that has knurling, you can continue to train your support grip strength with a minimal risk of tearing a callus by using fat grips that are usually composed of rubber or silicone based compounds.
Like fat grip implements, kettlebells commonly lack knurling, and heavier kettlebells may have handles that are thicker than typical barbells and dumbbells. These qualities can be advantageous for training your grip with exercises such as the suitcase carry, which is a particularly useful loaded carry variation due to its ability to train much of the core musculature and hip abductor muscles simultaneously. However, heavy kettlebells are not widely available, in part due to their high cost, so more experienced lifters may be confined to performing longer duration sets with kettlebells that focus more on grip endurance.
Pinch Grip Training
While the efficiency of being able to modify many lifts you are already performing into effective grip training exercises is distinct to fat grip attachments, pinch grip exercises share much of their benefits with the added advantage that you do not need to buy specialized equipment. If you wish, you certainly can purchase specialty devices such as pinch blocks, but you can train the same type of exercise with widely available weight plates.

A variety of different weight plates exist with varying thicknesses and textures that will affect how challenging grasping a particular load with a pinch grip will be. With a thick rubber bumper plate, a single plate may be sufficiently difficult for many lifters to hold with a pinch grip, while multiple plates may be required if using thinner iron plates or if an experienced lifter no longer finds a single 45lb (20.4kg) bumper plate to be challenging.

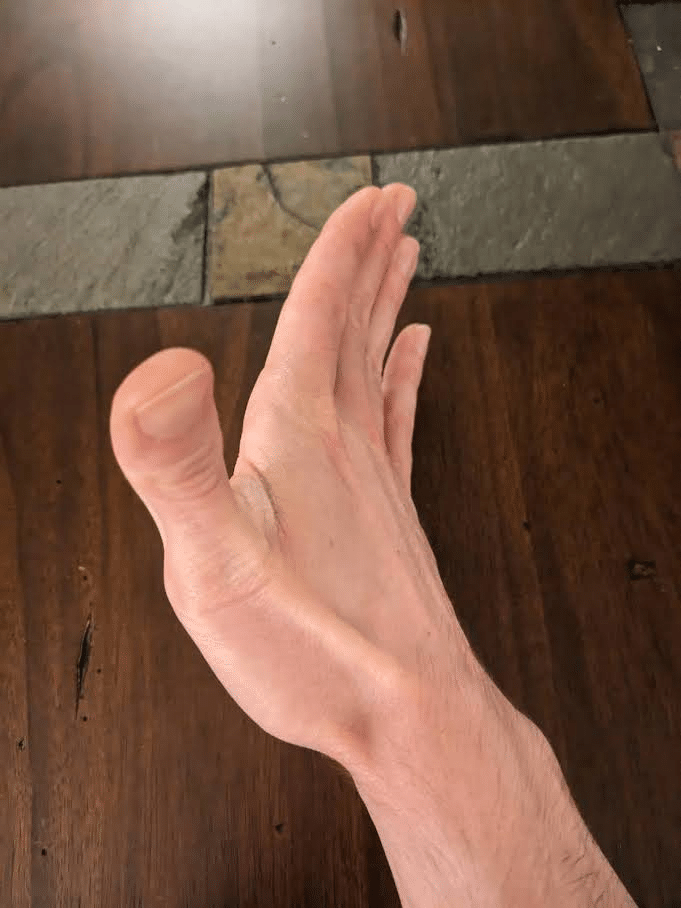
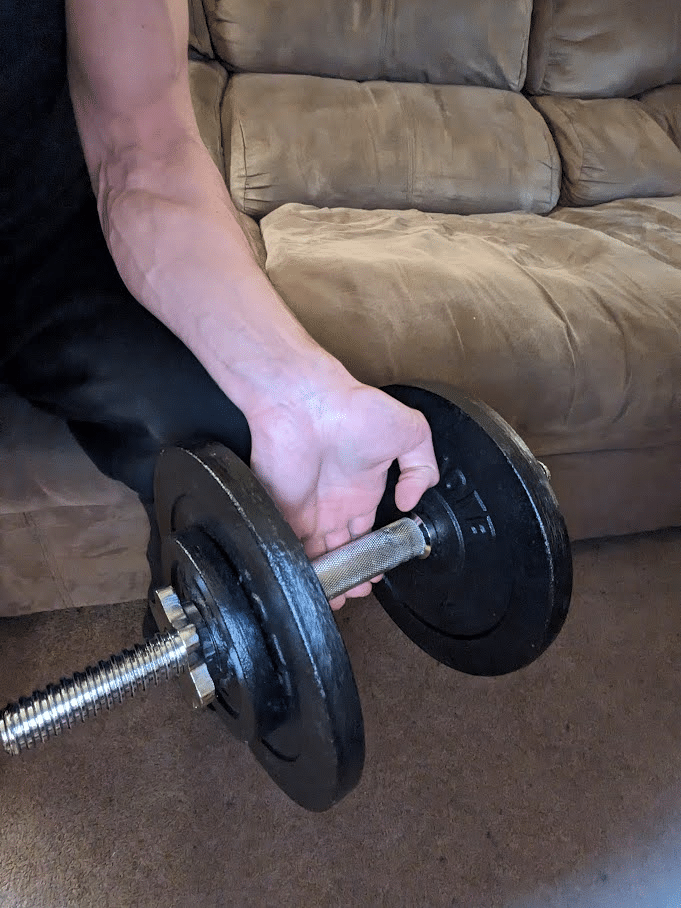
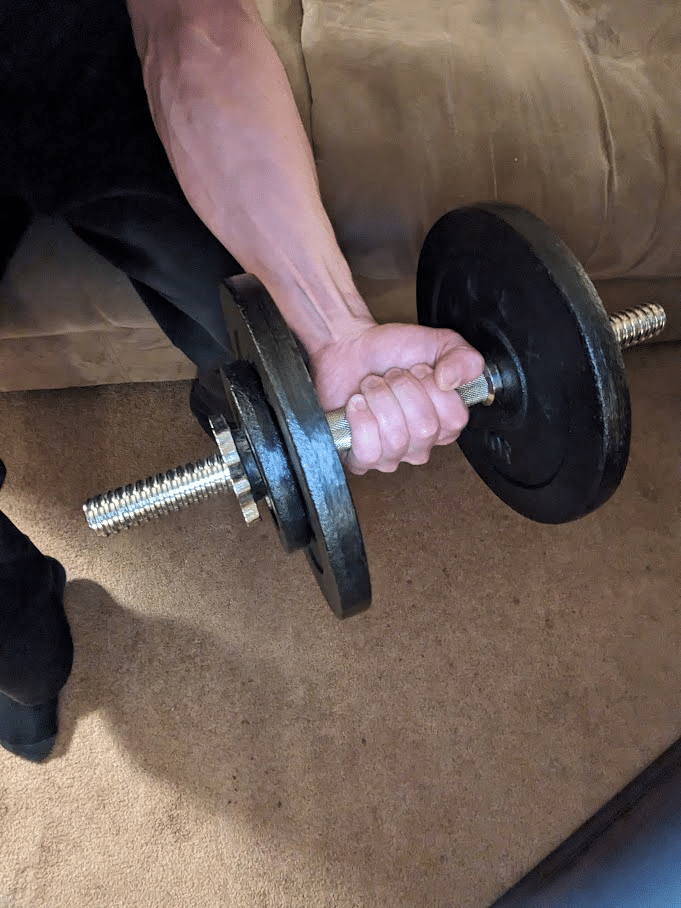
Pinch grip exercises can also be performed with a dumbbell by holding it with your fingers spread apart (i.e. abducted) around one end of the weight as the other end of the weight is directed toward the ground. This open-hand pinch grip exercise is quite humbling, and you will be limited to using light dumbbells that normally provide no challenge to your grip strength when grasping their handles. As the weight of a dumbbell increases, the difficulty of this exercise will assuredly increase from the greater load, but the greater diameters that heavier dumbbells typically have relative to lighter dumbbells can make an even more profound difference in the challenge. While hand size and finger length affect performance in a variety of grip exercises, these morphological characteristics are particularly impactful in dictating which dumbbells an individual can use for this pinch grip exercise (59,64). You may have world-class grip strength but be simply incapable of holding a 25lb (11.3kg) dumbbell in this manner if your fingers are physically not long enough to contact the sides of the weight. In addition to fixed load dumbbells that increase in diameter as they increase in weight, adjustable plate loaded dumbbells may also be used for this pinch grip exercise with the right setup.
When an adjustable plate-loaded dumbbell is normally loaded with a light weight, the sleeve may prohibit you from grasping the plate. However, if you apply a collar to one end while leaving enough space between the shaft and the collar before adding a weight plate and another collar, the sleeve may no longer prevent you from grasping it with an open-hand pinch grip. When performing a pinch grip exercise with either a dumbbell or a plate with a raised lip, a subtle shift in finger position can meaningfully influence how difficult holding a given weight will be. Grasping the dumbbell with your distal phalanges directly on the sides of the weight without the middle phalanges contacting the weight will be most challenging. Holding the dumbbell within your distal interphalangeal joints such that your distal phalanges are closer toward the bottom surface while your middle phalanges wrap around the top aspect of the side surface will be comparatively less difficult. Similarly, a plate pinch exercise will be easier if you are able to wrap your distal phalanges under a plate’s raised lip relative to if you are holding onto the flat surface.


Relative to most support grip exercises with standard diameter shafts, pinch grip exercises will impart lower axial loading, stress the hand skin to a lesser degree, and train the finger flexor muscles at longer lengths. These three qualities are exhibited by many fat grip exercises, but they can be even more exaggerated with pinch grip exercises, especially with the aforementioned dumbbell variation. However, relative to fat grip exercises, pinch grip exercises are not as specific to improving support grip strength, and their ability to enhance other attributes besides grip strength are much more limited given the exercise variation constraints.
When incorporating pinch grip exercise into a program with either a plate or a dumbbell, integrating it into a unilateral carry is a quality option if adequate space is available. Given its load constraints, this type of carry will not provide the same stimulus to the core or upper back muscles that a heavy dumbbell suitcase carry can. Nonetheless, brisk walking is beneficial in its own respect for increasing energy expenditure and providing general health benefits, particularly if your gym workout is your main form of physical activity in an otherwise fairly inactive day (96,201). When performing sets of pinch carries until grip fatigue, the unilateral variation may help reduce the risk of dropping a weight on your foot. With the pinch grip, a slight downward movement of the weight as fatigue and/or sweat accumulates can cause the weight to start rapidly slipping out of your hand. If this happens, having a free hand allows you to guide that weight to the ground so that it does not accidentally drop. Having any perspiration on your hands can negatively affect performance for any type of grip exercise, but its effect is disproportionately greater for pinch grip exercises that are totally reliant upon how much friction force you generate. Consequently having a towel to dry your hands and/or chalk can make a considerable difference if you have been working up a sweat during your session.
Wrist Extension Exercise


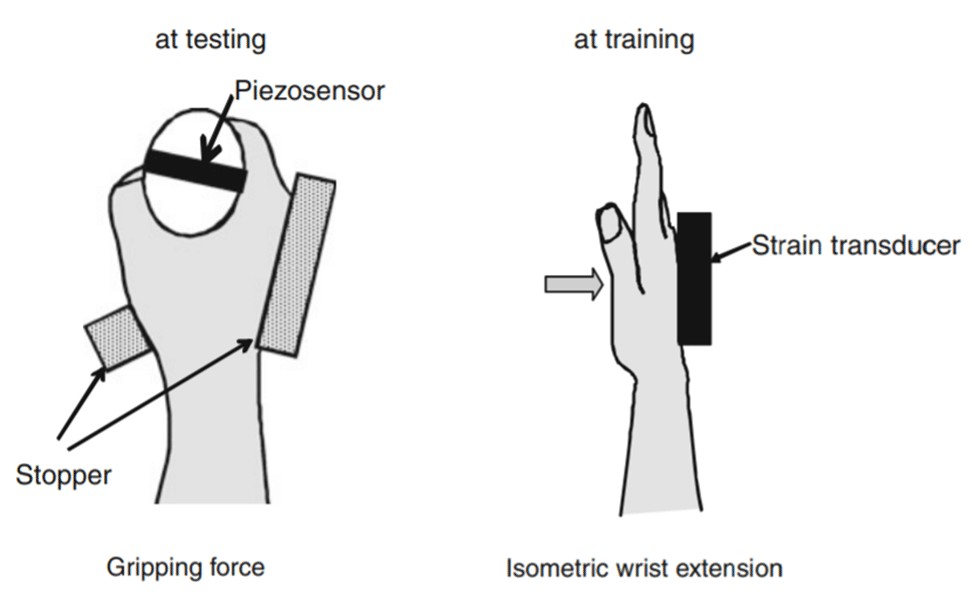
Relative to the previously covered grip exercises, the benefit of wrist extension exercise for someone who wishes to improve grip strength is not particularly intuitive. None of the wrist extensor muscles function as finger flexors like three of the wrist flexor muscles do. However, increasing wrist extension strength can nonetheless transfer to improved grip force as demonstrated by a resistance training intervention that Shiomose et al (2011) conducted. After assessing baseline grip force, the researchers assigned 13 untrained subjects to perform one set of wrist extension exercises five times per week for eight weeks with their right hands while their left hands served as controls (180). Each set involved 30 two-second isometric wrist extension reps with an intensity equal to 70% of the subject’s maximal voluntary contraction output, two-second inter-rep rest intervals, and a neutral wrist position (which was the same position where wrist extension strength was also tested). After the intervention, mean maximal gripping force increased in the trained limb by 19.2% and maximal wrist extension force increased by an impressive 90.9%. For strength athletes, it is worth noting that grip strength was tested during this study with a circumference of 6.1” (155mm), which is larger than the 3.6” (91mm) circumference of the typical barbell.
The wrist extensor muscles can help the flexor digitorum superficialis, flexor digitorum profundus, and flexor pollicis longus operate at favorable muscle lengths where they can generate maximal finger flexion force (184). Force is actively produced by a muscle through the cyclic formation of actin-myosin cross bridges within its sarcomeres, which are the functional units of its muscle fibers. Relative to moderate lengths, fewer cross bridges can form at short lengths, so active force production is submaximal in a shortened sarcomere position.
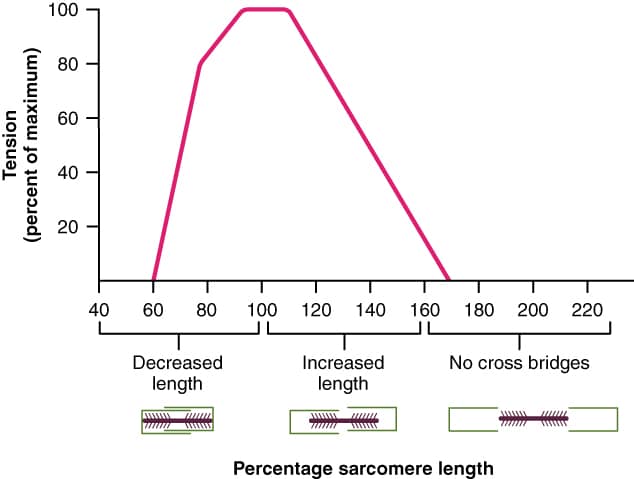
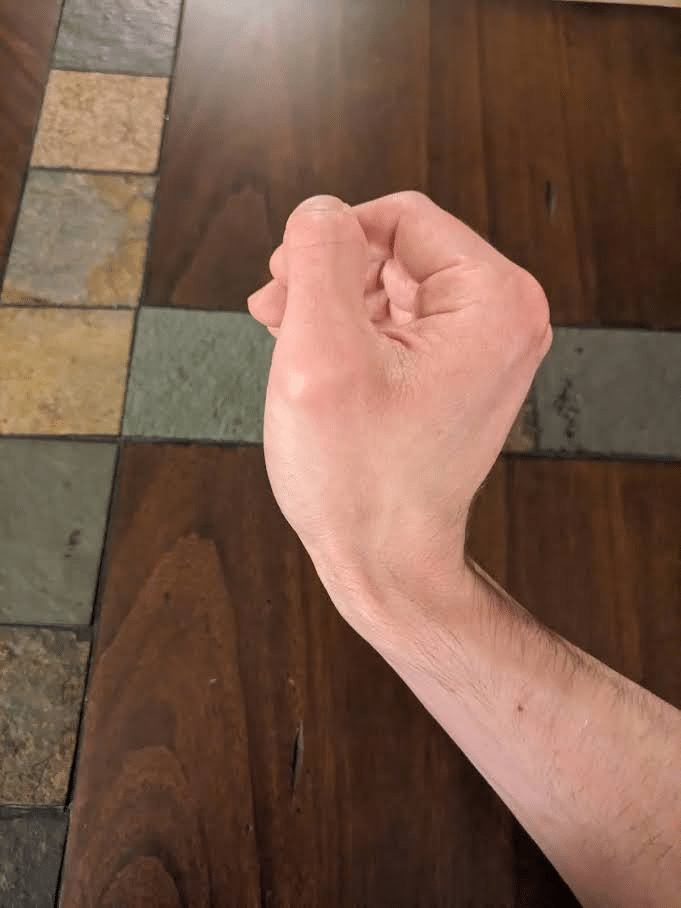
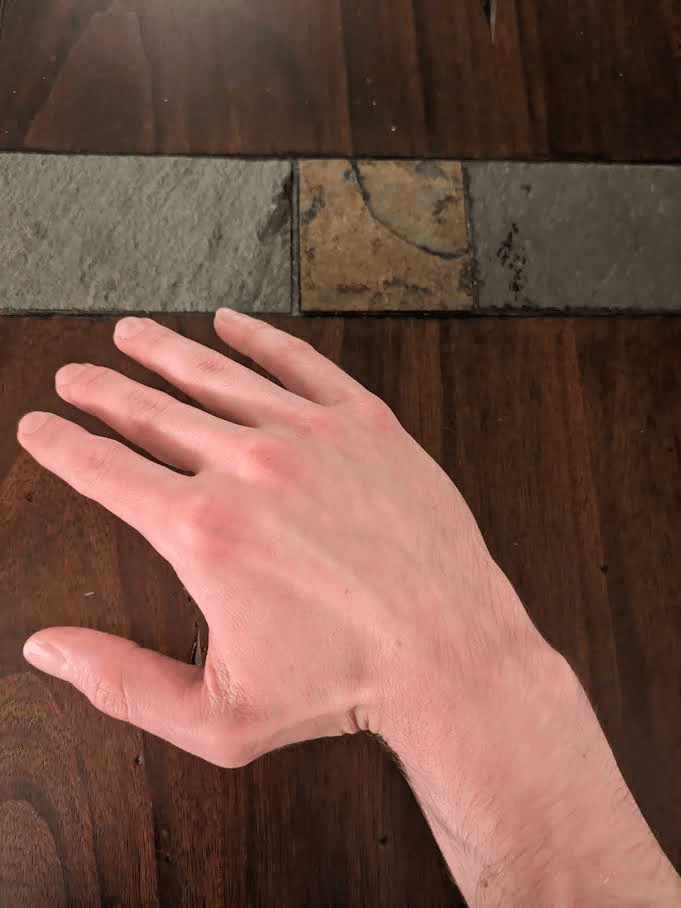
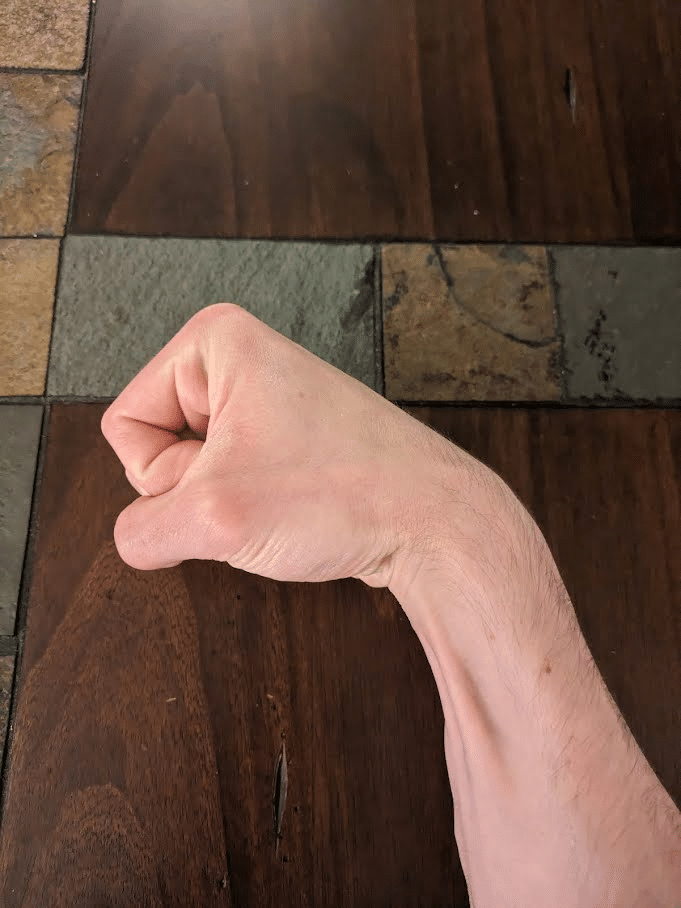
If the wrist maintains a neutral position when the fingers are in a flexed position, the flexor digitorum superficialis, flexor digitorum profundus, and flexor pollicis longus are shortened and consequently will not be able to generate maximal force. Given this relationship, maximal grip force is normally produced in an extended wrist position, which research has typically found to be about 20-45° beyond neutral (112,143,180). As the diameter of the implement that someone grips increases, the optimal wrist angle for generating grip force tends to be less extended (143). This likely occurs because thicker implements will allow the extrinsic finger flexor muscles to operate at longer lengths compared to thinner implements. When making a fist as forcibly as you can, you will likely notice that your wrist naturally moves into this mildly to moderately extended position. If you initially flex your wrist before making a fist, it is evident that grip force is submaximal in this position.
Maintaining the optimally extended wrist position during an intense crush gripping effort is not necessarily an easy feat because the flexor digitorum superficialis, flexor digitorum profundus, and flexor pollicis longus generate wrist flexion torque as they flex the fingers. Overall these three muscles have similar leverage at the wrist joint as the wrist extensor muscles do (69). However, their cross sectional area is greater than all of the wrist extensor muscles combined primarily due to the size of the flexor digitorum superficialis and flexor digitorum profundus (69). Compounding this size difference, only some of the wrist extensor muscles are well suited to assist with gripping since over half of the wrist extensor muscles also function to extend the fingers (62). Maximally activating the finger extensor muscles while gripping would be biomechanically inefficient because their force would partially be counteracting finger flexion force.


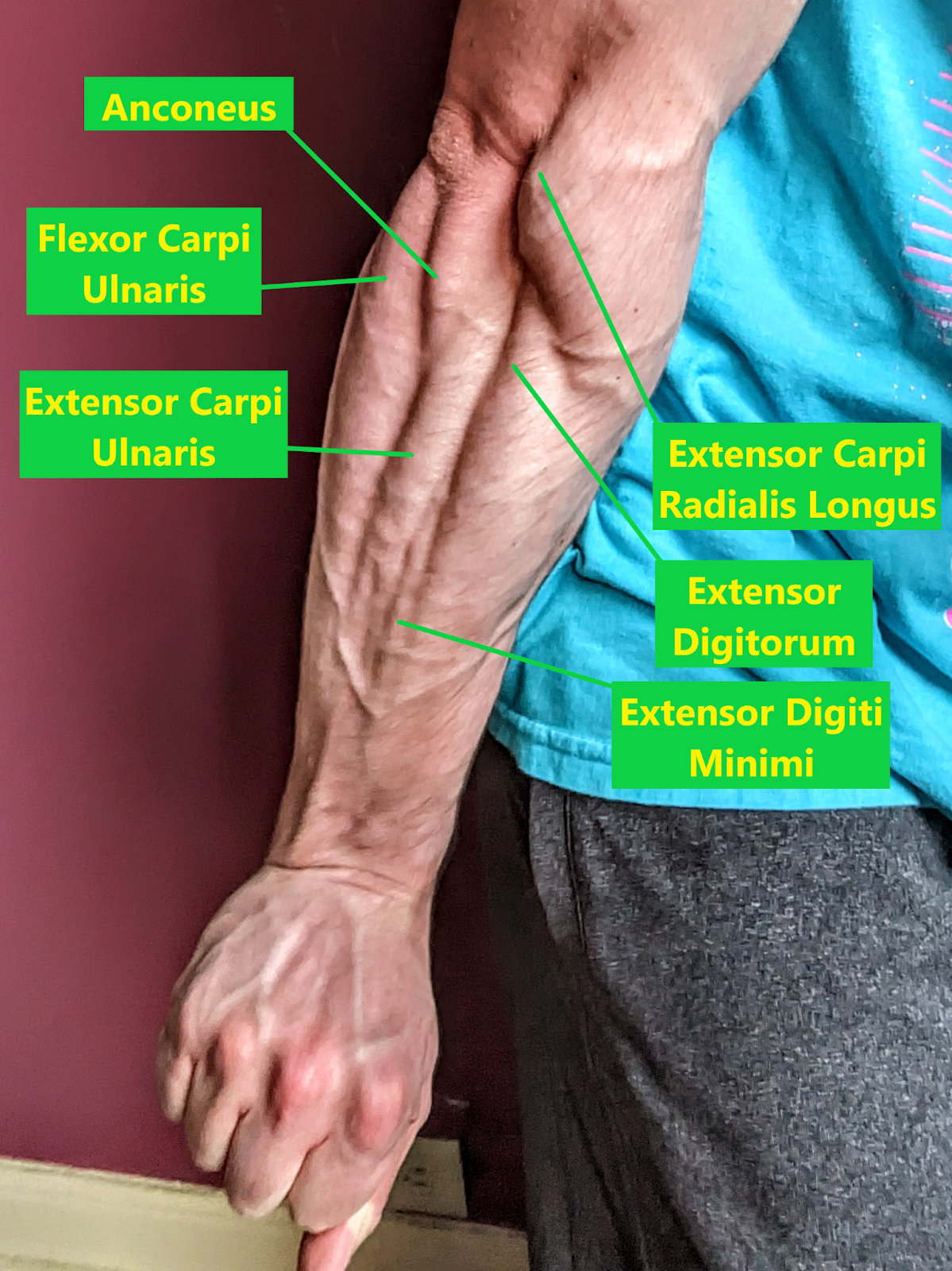
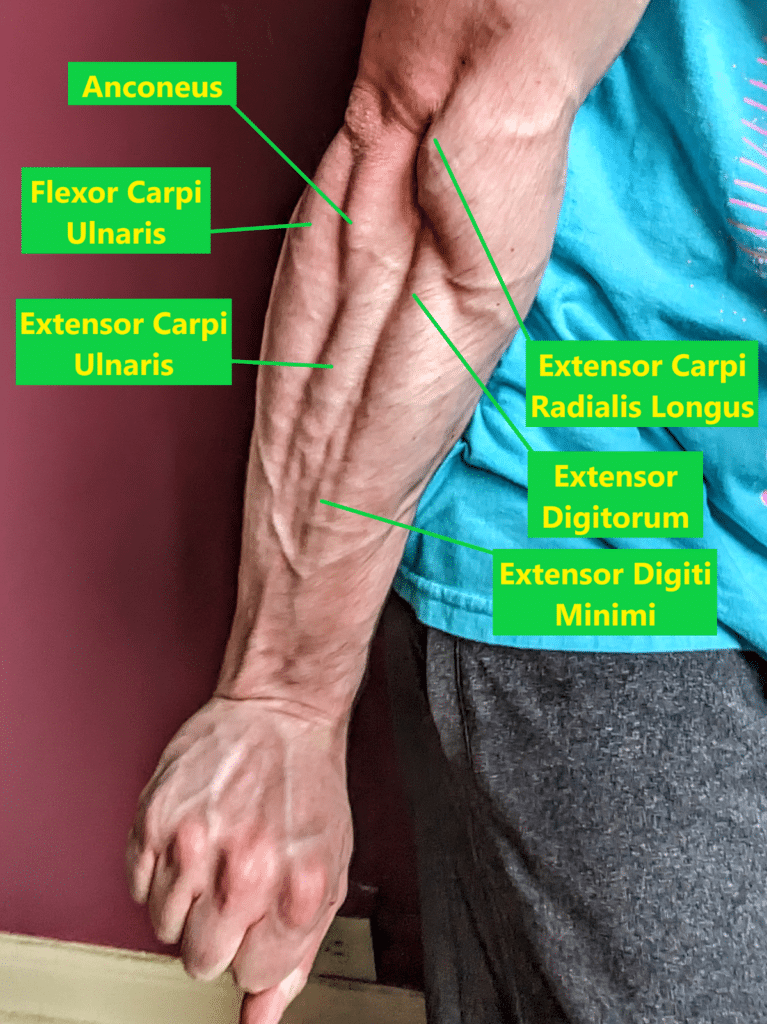
Several muscles contribute to wrist extension, but only the extensor carpi radialis longus, extensor carpi radialis brevis, and extensor carpi ulnaris can meaningfully do so without inadvertently producing finger extension torque (17,62,69). Together, the cross-sectional area of these three muscles is less than half that of the flexor digitorum superficialis and flexor digitorum profundus combined (9,69). Consequently, these three wrist extensor muscles can be quite challenged in maintaining the most advantageous wrist position during a maximal crush grip bout. If these three muscles are weak, someone may rely upon greater contributions from the other wrist extensor muscles (which also extend the fingers) to keep the wrist extended while crush gripping, which would result in lower grip performance due to their actions at the fingers. Before and after the intervention, Shimose et al measured EMG activity of the extensor carpi ulnaris and extensor carpi radialis muscles during maximal gripping and found their activity to increase significantly. In contrast, EMG activity of the extensor digitorum (which functions as an extensor for both the wrist and fingers) while gripping did not increase following the intervention.
In light of the findings from Shiomose et al (2011), it is quite plausible that wrist extension exercise can transfer to improved grip performance, but the degree of carryover likely varies depending on the type of gripping. Beyond measuring grip force, the researchers also measured “grip strength” as a distinct variable, which I initially found confusing. Grip force was measured with a device called a piezosensor at 16 different fixed wrist positions in 10° increments ranging from 70° of flexion to 80° of extension. Of these 16 force measurements, the greatest was considered to be maximal grip force. Generally, grip force and “grip strength” are used as interchangeable terms, but the researchers additionally tested “grip strength” with a dynamometer where participants used whichever wrist position they freely selected. While the difference reached statistical significance, “grip strength” only increased by 1.4% after 8 weeks of training in contrast to the 19.2% increase in “grip force.” From my interpretation of the text, the authors did not discuss any potential reasoning underlying this discrepancy.
Potentially, participants may have self-selected wrist positions where their grip force was submaximal during “grip strength” testing with the dynamometer. Based on the graphical depiction of how participants’ grip force varied with wrist angle, it is apparent that the wrist extension training yielded the smallest effects in wrist positions that were very extended or flexed. If participants self-selected wrist positions that were suboptimal for generating grip force, they may have failed to see much of a change in “grip strength” with the dynamometer. If this occurred, the values for “grip strength” would not have reflected the participants’ maximal potential grip force that could have otherwise been measured with the wrist closer to a neutral position.
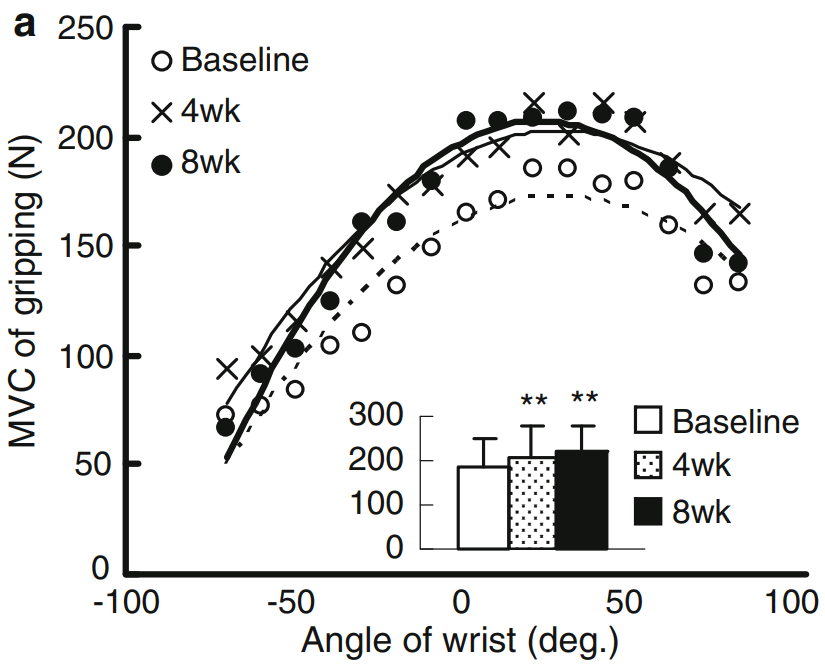
When thinking about potential carryover to a heavy support grip exercise like the deadlift, it is worthwhile to consider the constraints it imposes on wrist position. Given the gravitational forces acting on the load being lifted, it simply is not feasible to maintain an extended wrist position to any notable degree during this type of gripping exercise. In contrast, the wrist is free to move into an extended position where the finger flexor forearm muscles may generate maximum grip force during a crush grip exercise, which is not resisted by gravity. Consequently, I deem the grip force changes tested by Shiomose et al (2011) with wrist position constraints to be more relevant to support grip carryover than the “grip strength” that was tested without wrist constraints. From the figure published in their article, it is clear that the wrist extension training intervention increased grip force in a neutral wrist position. While the difference did not reach statistical significance due to meaningful inter-subject variability, the mean wrist position where maximal gripping force was produced also shifted from 34° to 25° of extension. For individuals who wish to express maximal grip force in heavy support grip exercises, this trend toward a neutral wrist position for generating max grip force is advantageous. As depicted by the figure above from Shiomose et al (2011), mean grip force was quite similar when tested from 0-50° degrees of wrist extension after the intervention. While we previously covered the mechanism by which wrist extension training can transfer to grip strength without wrist position constraints, it is presently unclear to me specifically how carryover occurs to gripping when the wrist positions are fixed. With constrained wrists, the production of wrist extension torque cannot influence the length tension relationship of the finger flexor forearm muscles. More remains to be investigated about how wrist extension training may transfer to grip performance, but its potential value is promising nonetheless.
If strengthening the wrist extensor muscles can contribute to enhanced grip strength, fatiguing them should acutely impair grip strength, which is what Souza et al (2017) reported to occur (186). In their study, participants tested their maximal crush grip strength with a dynamometer before and after performing a set of wrist extension exercises loaded with 75% 1RM until fatigue. In contrast to if dumbbells or barbells were used, the participants performed wrist extension exercise with a strap that circumvented the need to grip the weight, which could have otherwise directly induced some finger flexor muscle fatigue. Following the wrist extension exercise, crush grip strength was 16% lower than beforehand, providing further evidence in support of how the wrist extensor muscles contribute to grip strength.
Forearm Muscularity
The focus of this article has been on improving grip strength for performance, but the methods discussed can also be directly relevant to lifters who simply wish to just visibly look more muscular. With the exception of the face and neck muscles, the forearm muscles are visible more often than nearly any other muscles in the body since they can be directly seen when wearing a short-sleeve shirt. Relative to any other wrist or hand movement, wrist flexion exercise will train the greatest amount of muscle mass, so I consider wrist curls to be the most efficient type of exercise for enhancing forearm muscularity. Wrist extension exercise is also useful for this objective, but its ability to stimulate increases in total forearm mass will be lower due to the size discrepancy between the muscles in the anterior and posterior compartments of the forearm. Increasing the size of the wrist flexor muscles by 50% would add approximately as much muscle mass as doubling the size of the wrist extensor muscles (9,69). Nonetheless, wrist extension exercise is quite easy to add into a program as a minimally fatiguing antagonist superset with wrist curls, whether performed at a gym or at home with moderately light dumbbells. With an antagonist superset, you would perform a set of wrist extension exercise immediately after completing a set of wrist curls or vice versa. These exercises can also be readily incorporated into non-competing giant sets (performing three or more sets of distinct exercises in succession that train different muscle groups) with other accessory exercises to increase your time efficiency. Whenever we consider adding new exercises into an existing program, time constraints must be considered so use of non-competing giant sets is a strategy I strongly recommend employing for a variety of different muscle groups.
As with hand grippers, I recommend initially using loads for wrist exercises that allow you to train in a moderate to moderately high rep range, such as somewhere within the span of 10-25 reps per set. During each rep, you are only moving the weight a small distance compared to most other exercises, and some individuals may experience wrist discomfort if they load their wrists in deep ranges of wrist flexion and extension with higher loads if they are not accustomed to doing so (36,97). However, a rather wide range of reps can induce similar hypertrophic responses on a per set basis if sets are taken sufficiently close to failure, so feel free to try out different rep ranges (173). While selecting weights for wrist flexion and extension exercises, it is worth noting that wrist extension strength has been measured to be 57-60% of wrist flexion strength on average (46,121,216). When performing wrist flexion and wrist extension exercise supersets, you can use the same dumbbells for each if you train flexion in the higher end of the 10-25 rep range and extension in the lower end. Alternatively, you can just use different dumbbell loads for supersets, but that may not always be practical in a busy gym where you have to share equipment or time-efficient if using a pair of plate-loaded dumbbells at home.
With respect to training volume, your proximity to failure per set, rest intervals, exercise selection, sleep, diet, genetics, sex, stress levels, and recent training history may all influence how many sets per week are optimal for inducing muscle hypertrophy. For some populations, low volume training can induce significant hypertrophy, but training volume exhibits a dose-dependent positive relationship with muscle hypertrophy up to a certain point (174). Where that point lies for you as an individual is not necessarily easy to determine, especially since optimal volumes may differ among muscle groups and change over time even within the same person. As training volumes rise, they also impart diminishing returns on hypertrophy, so plenty of lifters may not prefer to invest disproportionate time training to chase that increasingly small benefit that separates quite effective from optimal. With all of this said, performing at least 10-12 quality sets per muscle group divided over 2-3 sessions is a sensible approach for muscle groups that you prioritize developing based on the available data (18,174).
However, relative to how many muscles in the human body lifters may wish to develop, the research investigating the relationship between volume and hypertrophy is fairly limited. In addition to measurements of changes in full body lean mass, studies have investigated the quads, triceps, biceps, hamstrings, and trapezius (with the latter two muscle groups having very limited research) (18,174). To my knowledge, no research has assessed how hypertrophy of any forearm muscles is affected by training volume as is the case for most muscles. Beyond any potential differences in how these muscles may respond to volume compared to those that have been studied, quantifying training volume can be a challenge for the forearm muscles that function as finger flexors. These muscles may be quite active during many exercises, and we simply lack any evidence that could inform us about how efficiently isometric gripping exercises can develop these muscles. While the flexor digitorum superficialis and flexor digitorum profundus constitute a meaningful proportion of total forearm muscle mass, the finger flexor muscles still do not comprise the majority of forearm muscle mass (31).
If you prioritize increasing forearm muscle size for the purpose of having more visibly muscular forearms and do not have grip strength goals, I am unaware of any advantage that gripping exercises have over dynamic wrist exercises. When wrist curls are performed with the previously discussed finger flexion technique, they will train all of the finger flexor muscles involved with gripping exercises in addition to other forearm muscles only effectively trained with wrist exercises. Gripping exercises may yield higher activation of the wrist extensor muscles than wrist curls, but I have little doubt that any type of exercise can develop these muscles more effectively than direct wrist extension exercise (129). With this said, gripping exercises can certainly serve a role in a program for someone who strives to induce forearm muscle hypertrophy without caring about grip strength. Especially in the long-term, exercise variety can be psychologically refreshing and help you enjoy training. Utilizing wrist flexion and extension exercises is just the most direct way to increase forearm muscle size. Progressing to 10-12 weekly sets of wrist flexion and extension exercise may be a straightforward way to ensure that most of the forearm musculature receives a robust hypertrophic stimulus regardless of what else is in your training program. Increases in forearm muscle size can be achieved with lower volumes, but the aforementioned set range (divided over 2-3 weekly sessions) is a reasonable target if you really prioritize increasing forearm muscularity.
The Rest of the Forearm
Given that a clear majority of the muscles in the forearm either function as a flexor or extensor of the wrist, performing a combination of wrist flexion and extension exercise will train most of the forearm musculature. However, five muscles within the forearm, which collectively have a total mass close to one quarter of the total forearm muscle mass, do not cross the wrist joint and consequently will not be trained by wrist exercises (10,31). One of these muscles is the anconeus, which lies just below where the distal triceps tendon inserts on the bony prominence at the back of your elbow known as the olecranon. The small anconeus constitutes about 2.5% of the forearm’s muscle mass and assists the triceps in extending the elbow in addition to serving a role in stabilizing the elbow joint (10,31). Due to its function, any elbow extension exercise you use to train your triceps will also train your anconeus.
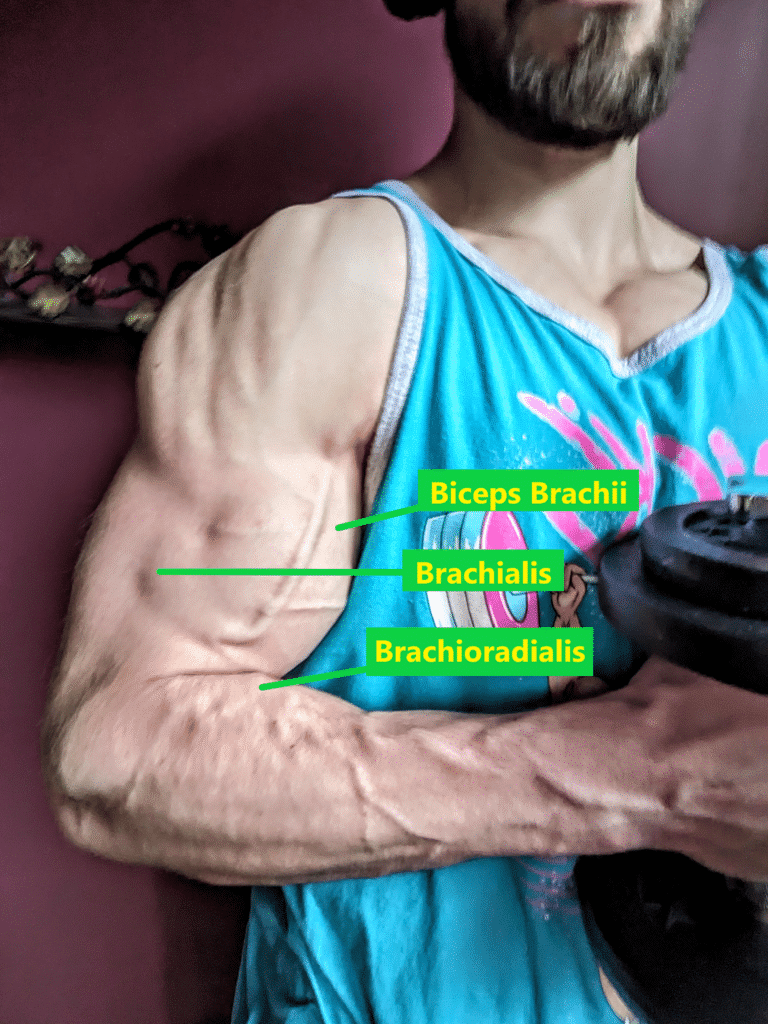
The largest of the muscles that do not cross the wrist is the brachioradialis, which has the greatest peak moment arm for generating elbow flexion torque of any muscle in the body (10,57,136,137,138). Consequently, it functions as a primary elbow flexor along with the biceps and the brachialis, which both have greater muscle volumes and cross sectional areas than the brachioradialis (10,137). All three of these muscles will be trained with any exercise that meaningfully resists elbow flexion such as variations of curls, vertical pulls, and (to a somewhat lesser degree) rows (68,119). Compared to using a supinated grip, I’ve previously heard lifters and researchers advocate that the brachioradialis can be trained to a greater degree with a neutral grip (e.g., hammer curl) when performing elbow flexion exercises (49,75). Some biomechanical research does indicate that the biceps has a mildly greater elbow flexor moment arm with a supinated forearm compared to a neutral forearm at certain elbow joint angles, but the same applies to the brachioradialis, which would still have greater elbow flexion leverage than the biceps with any forearm position (10,139). EMG research, which has its limitations, has also indicated that the brachioradialis exhibits similar or even greater activation when performing curls with a supinated grip compared to a neutral or pronated grip (27,37,40,66,105,106,190). While new evidence may emerge in the future suggesting otherwise, I am not presently under the impression that neutral grip exercises are superior to supinated grip exercises for developing the brachioradialis.
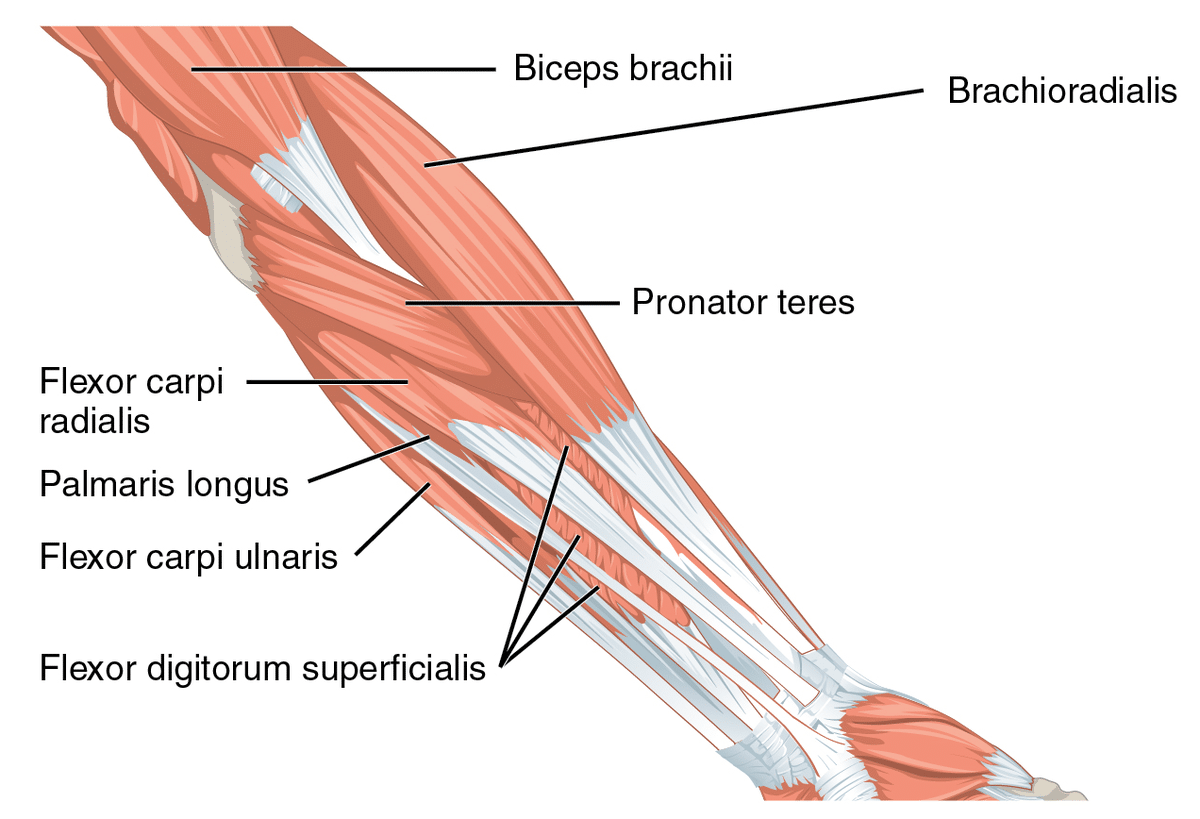
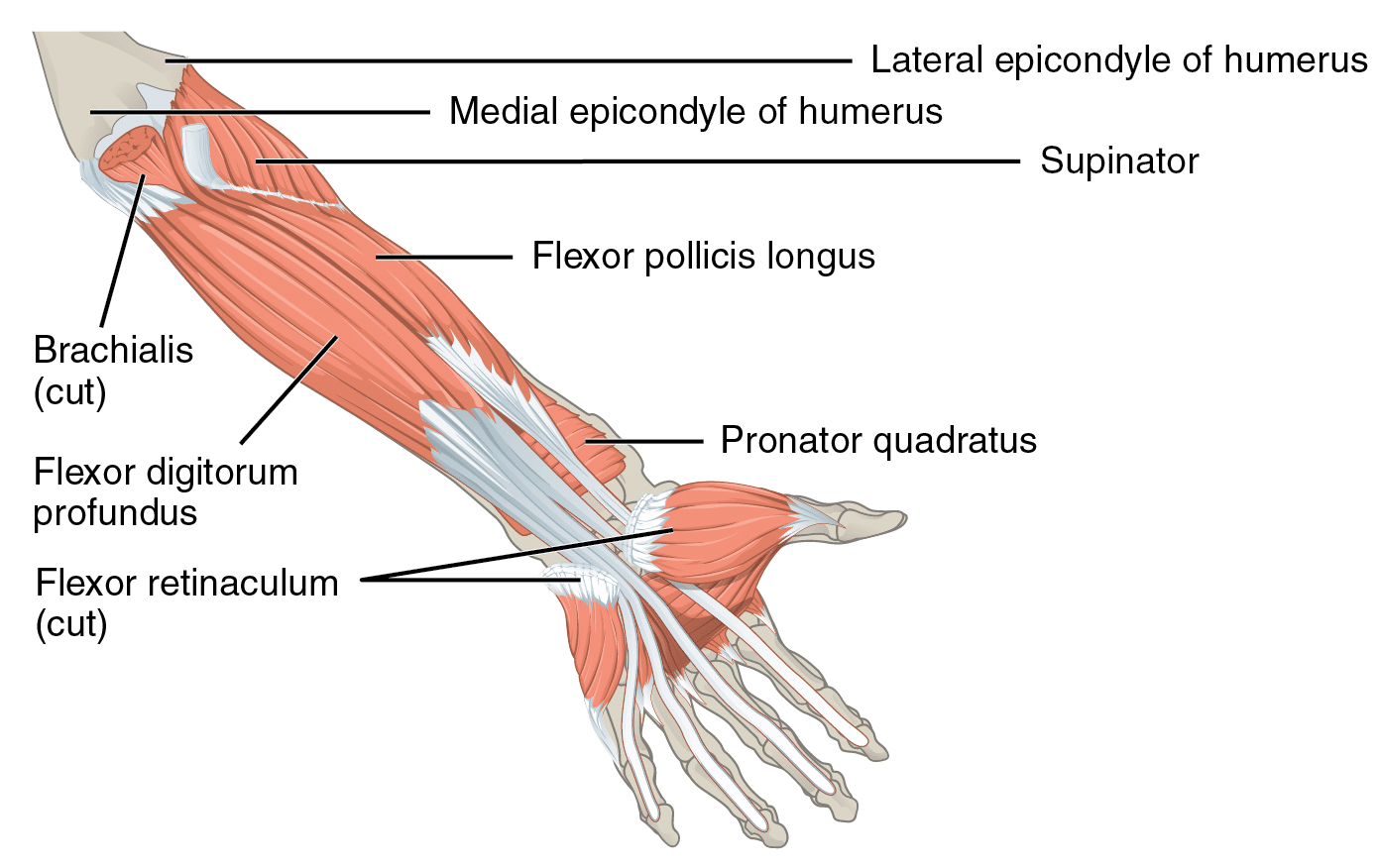
The forearm additionally contains the supinator, which functions as a primary forearm supinator along with the biceps, as well as the pronator teres and pronator quadratus, which both function as primary forearm pronators (32,57,70,73,139). To variable degrees, other previously discussed forearm muscles secondarily assist with supination and pronation, but they have greater leverage to perform different actions such as wrist flexion or extension (32,57,69,73,139,162). Elbow flexion exercises will train the biceps (and to a lesser degree the pronator teres), but people rarely perform exercises that directly resist pronation and supination (162,190). Consequently, the primary forearm pronators and supinators may not be particularly well developed for many lifters with the exception of the biceps. In terms of aesthetics, their lack of development would not be easily detected since together they contribute to a little over 10% of the total muscle mass contained within the forearm and hand (31). Except for arm wrestling, pronation or supination strength is also unlikely to have a direct influence on performance in most strength sports. Given the lack of research on the topic, I will not claim that performing pronation or supination exercises will reduce the risk of sustaining any injury, but it is biologically plausible that these exercises can enhance active joint stabilization and the load tolerance of tendons. For instance, the pronator teres may assist the wrist flexor muscles and ulnar collateral ligament in stabilizing the elbow joint (which is particularly relevant to baseball pitchers), and its tendon is commonly involved with golfer’s elbow (84,147,151,176,200,208).
If you wish to perform pronation or supination exercise, an asymmetrical weight is a useful tool for doing so. An adjustable dumbbell with plates loaded only on one side, a sledgehammer, or a bat can be used to train dynamic pronation and supination in an alternating fashion where you cyclically move from full pronation to full supination. On average, supination strength exceeds pronation strength, so you’ll most likely fail the pronation half of this exercise before the supination half (12). To train the supinators as effectively as the pronators, you can simply finish the set with pure supination reps by alternating between pronated and neutral positions. Since there are considerably more impactful exercises that merit a greater proportion of training time, I would generally recommend treating pronation and supination exercises like other commonly neglected movements if you opt to train them. Performing 1-2 sets twice per week should be sufficient to reap the potential benefits of these exercises in a time-efficient manner unless you have a more specific need (e.g., are a competitive arm wrestler or are rehabbing an injury).

As mentioned in the wrist anatomy passage, the wrist joint enables radial deviation (AKA abduction) and ulnar deviation (AKA adduction) in addition to flexion and extension, which we already discussed in detail. Like forearm pronation and supination, radial deviation and ulnar deviation exercises can be trained with an asymmetrical weight, such as a hammer or an adjustable dumbbell loaded only on one side. Alternatively a band may be used for wrist deviation exercise. Unsurprisingly, a combination of radial deviation, ulnar deviation, wrist flexion, and wrist extension exercises can effectively train more forearm muscles than exclusively using wrist flexion and extension exercises. However, the addition of wrist deviation exercises provides notably diminishing returns due to the overlapping wrist functions exhibited by forearm muscles.




The majority of muscles that can meaningfully contribute to radial or ulnar deviation also function as wrist flexors or extensors (69,162). Two muscles that insert onto the thumb, the abductor pollicis longus and extensor pollicis brevis, are exceptions. These two small muscles that constitute about 3.5% of the total muscle mass in the forearm and hand, function as primary radial deviators but cannot meaningfully contribute to generating wrist flexion or extension torque (31,69,162). In contrast, a combination of wrist flexion and extension exercises can train the other forearm muscles that function as radial deviators or ulnar deviators. For instance, the extensor carpi radialis longus and extensor carpi radialis brevis function both as primary wrist extensors and radial deviators. Similarly, the flexor carpi ulnaris and extensor carpi ulnaris function as ulnar deviators but also respectively contribute to wrist flexion and wrist extension. Consequently, radial deviation and ulnar deviation exercises are not required to train most of the muscles that contribute to these actions. If you are striving to achieve every gram of forearm muscle mass you can possibly attain or have a more specialized goal, wrist deviation exercises can serve a role. However, they would be a very low priority for many lifters given that training time is finite.
Resistance Training Intervention Effects on Grip Strength
In light of what we have covered thus far, it is quite reasonable to hypothesize that resistance training interventions consisting of exercises for all four wrist movements along with forearm pronation and supination would increase grip strength. Hughes et al (2004) and Szymanski et al (2004, 2006) conducted three similar studies where they respectively assigned collegiate baseball players to 6-week interventions or high school baseball players to 12-week interventions (78,194,195). Their control groups performed common resistance exercises (including squat, bench press, and deadlift), while their experimental groups performed the same lifts in addition to exercises training the four wrist motions along with forearm pronation and supination. After the two 12-week interventions, crush grip strength increased by similar degrees for each group, while neither group significantly increased crush grip strength after the 6-week intervention. In each study, Szymanski et al also tested 10-rep maxes for the four wrist movements along with forearm pronation and supination before and after the interventions. Predictably, the experimental groups that performed two sets of 8-12 reps for each of the six movements three times per week experienced significantly greater 10RM increases for each movement relative to the control groups. Given the major roles the flexor digitorum muscles serve in generating wrist flexion torque, the lack of superior grip strength improvement from the groups performing barbell wrist flexion exercise may be somewhat surprising. While these results indicate that performing wrist exercises will not automatically increase any type of grip strength, they do not mean that wrist exercises are pointless for individuals who wish to improve grip strength.
Supplemental exercises that are programmed with the intent to induce hypertrophy of muscle groups that function as prime movers in other lifts do not necessarily provide immediate carryover to those different lifts. For instance, a powerlifter may complete an 8-week mesocycle of offseason training that prioritizes progression on 8-12 rep sets of high-bar pause squats, Romanian deadlifts, and bent-over rows but lacks competition-style deadlifts. The lifter may significantly increase the load used for those exercises over time but fail to experience any 1RM increase in the deadlift if it is tested directly following that block. By no means would this result indicate that those three exercises are worthless to a powerlifter striving to enhance his/her deadlift max. In isolation, the supplemental exercises may not necessarily yield immediate performance transfer. However, they may nonetheless be valuable components of a long-term training program if they help increase the size of the deadlift’s prime movers. A period of training the deadlift can subsequently allow a powerlifter to have the increase in strength potential from the supplementary exercises manifest as an actual performance improvement.
Similarly, a block of wrist exercises has the potential to potentiate greater grip strength improvements if specific grip exercises are trained afterwards. Alternatively, performing wrist exercises during a training block that includes some high-intensity grip exercises has the potential to yield greater grip strength increases compared to if only the grip exercises are utilized. Furthermore, utilizing the previously discussed dynamic finger flexion technique with wrist curls may also positively influence carryover to grip strength compared to the standard wrist curl technique used in the three intervention studies.
No study has assessed an intervention with finger flexion wrist curls, but one study has assessed a resistance training intervention exclusively involving dynamic finger flexion exercise for the index through little fingers. Shim et al (2008) assigned 33 untrained young adults to a control group that did not train or experimental groups that followed six-week programs consisting of dynamic finger flexion exercise performed for six sets of 10 reps with 70% 1RM three times per week (179). Three different training groups were assessed, one of which performed the exercise with the four fingers simultaneously, while the other two groups trained each finger independently. Of the two independent finger training groups, one group was directed to try to restrict movement of the non-training fingers during the exercise, while the other group did not receive this direction. Shim et al did not test the participants’ “grip strength,” but they did test the maximal isometric flexion force that they could generate with the four fingers simultaneously while the hand, wrist, and forearm were stabilized with braces. In contrast to the control group, each training group similarly increased maximal finger flexion force after six weeks by a combined average of 39%. With the absence of any thumb contribution, this outcome is not the same as the widely tested crush grip strength with a dynamometer. However, the magnitude of isometric finger flexion force produced by the index through little fingers determines most of the grip strength displayed with all five fingers engaged (38).
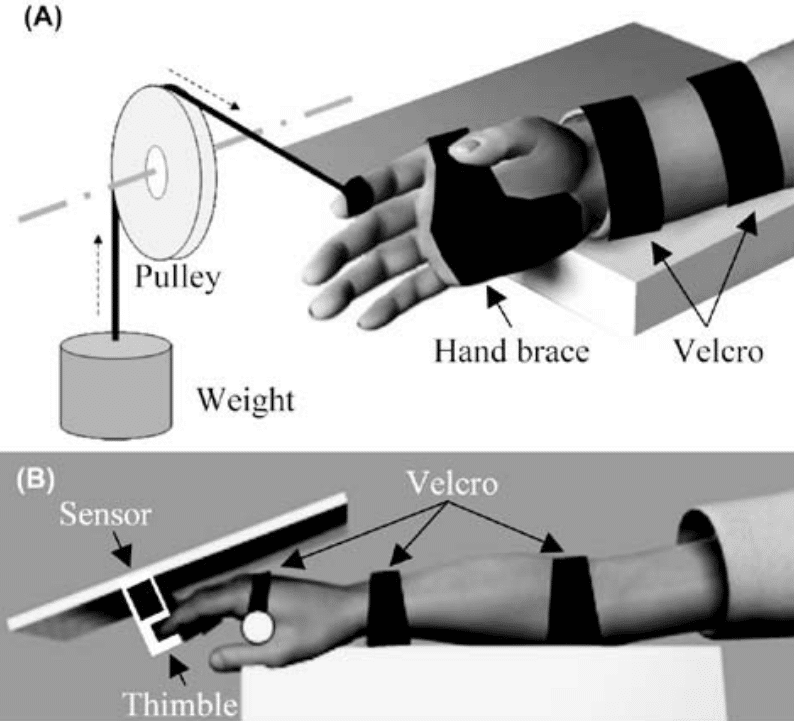
Just as crush grip strength is not the same as support grip strength, so too is the finger flexion strength tested by Shim et al not identical to the various types of task specific grip strength someone may wish to improve. Nonetheless, there is little reason to think that training methods that significantly increase isometric finger flexion force cannot transfer to enhanced potential strength performance when using grips reliant on this force. When assessing the information covered throughout this article thus far, finger flexion wrist curls can consequently be valuable components of a grip training program even if superior grip strength gains did not occur directly after interventions with wrist flexion exercise.
While searching for research on how different grip training protocols may affect changes in grip strength, I also found two studies that assigned untrained young adult participants to hand gripper exercise interventions. Berg et al (2018) designed a custom hand gripper device that allowed dynamic crush grip exercise to be incrementally loaded with a pulley (20). During a progressively overloaded six-week program, their participants performed four sets of four reps for the hand gripper exercise four times per week loaded with 90% 1RM. After the intervention, they increased their average dynamic hand gripper 1RM by 26.5%. Berg et al also performed forearm measurements and calculations to estimate forearm muscle mass in their participants. Their estimated forearm muscle mass was 2.8% greater following the intervention, but this difference was not statistically significant. In a lower intensity study, Sharma et al (2020) assessed changes in isometric crush grip strength tested with a dynamometer after two different six-week exercise interventions (178). The control and experimental groups both performed crush grip exercise with a squeeze ball for 10 reps of 10-second squeezes with 2-second inter-rep rest intervals three times per week. The experimental group’s participants also trained with a hand gripper (with 20kg of resistance) as they performed 10 reps with 2-second isometric actions in the contracted position three times per week. After the intervention, the experimental and control groups respectively increased their mean dynamometer grip strength by 26% (a statistically significant change) and 10.6% (not a statistically significant change).
Overall the findings from Berg et al and Sharma et al that hand gripper exercise interventions can enhance dynamic or isometric crush grip strength are unsurprising. While Berg et al and Sharma et al selected different grip strength outcomes measures, it is interesting to see that each of their experimental groups experienced essentially the same magnitude of grip strength improvement. By using a progressively overloaded intervention with higher intensities and set volumes than Sharma et al, I would have predicted that the experimental group from Berg et al would experience a greater degree of grip strength improvement. However, comparisons between studies using different outcome measures that reflect a similar construct should be taken with a grain of salt. Untrained participants may also respond differently than trained individuals, who may require more robust training stressors to experience improvements in strength.
Tennis Elbow and Golfer’s Elbow
While exploring many facets of grip training, it is worthwhile to cover the two most common types of grip-related injuries that affect lifters and the general population. The human body has a multitude of different tendons, but certain tendons are much more likely to develop tendinopathy, an overuse injury that fundamentally results from a tendon being repeatedly loaded beyond its load tolerance without adequate time to recover (128). Previously, the term “tendinitis” was used to describe this condition, but the suffix “-itis” denotes inflammation, which is not necessarily present in a pathological tendon (6,175). Alternatively, “tendinosis” may be used to describe structural degradation in the absence of inflammation, while “tendinopathy” can describe a tendon disorder more broadly and encompass pathological changes that precede degeneration (16). In addition to the pronator teres, four of the wrist flexor muscles (including the flexor digitorum superficialis) originate from the common flexor tendon at the humerus’ medial epicondyle (7). Similarly, four of the wrist extensor muscles originate from the common extensor tendon at the humerus’ lateral epicondyle, which also serves as an origin for the supinator (65). If you have your arms at your side with your palms facing forward (i.e., supinated), the medial epicondyle is the bony bump on the inside of your elbow, and the lateral epicondyle is the bony bump on the outside of your elbow.
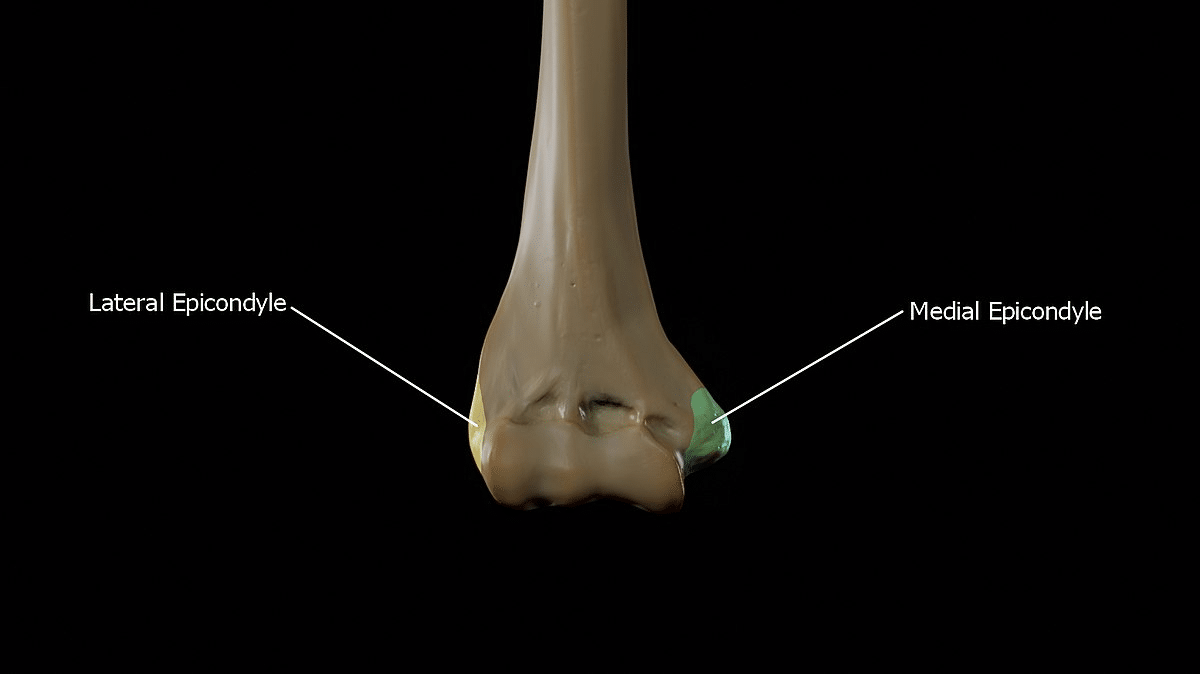
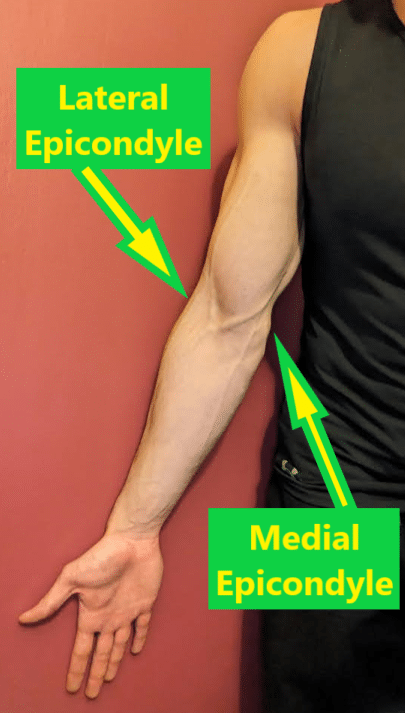
Golfer’s elbow and tennis elbow respectively refer to tendinopathy that develops at the medial epicondyle or lateral epicondyle, which clinicians commonly call medial epicondylitis or lateral epicondylitis (65). The tendons from other muscles (e.g., extensor digitorum) may be involved, but the common extensor tendon’s portion corresponding to the extensor carpi radialis brevis is most commonly affected with tennis elbow (142,172). On the other hand, the common flexor tendon’s portions corresponding to the flexor carpi radialis and pronator teres are often affected with golfer’s elbow, which may also involve diffuse injury throughout the common flexor tendon (145). These two injuries can result in notable elbow pain during and after activities which load these tendons, so they can become meaningful impediments to lifting and a variety of other athletic activities such as the sports for which they received their names. While grip training exercises can be quite painful as a result, other exercises that use the forearm muscles as stabilizers such as the bench press and back squat can also be rather provocative after the tendinopathy is aggravated. If a tendinopathy has reached a particularly irritable phase, even daily activities which impart low tendon loading such as holding a mug of coffee or opening a door can provoke pain (116). Once it has developed, tendinopathy can take a while to resolve, and continuing to load an injured tendon excessively beyond its tolerance can worsen the situation to the extent that it may become a chronic disorder (39).
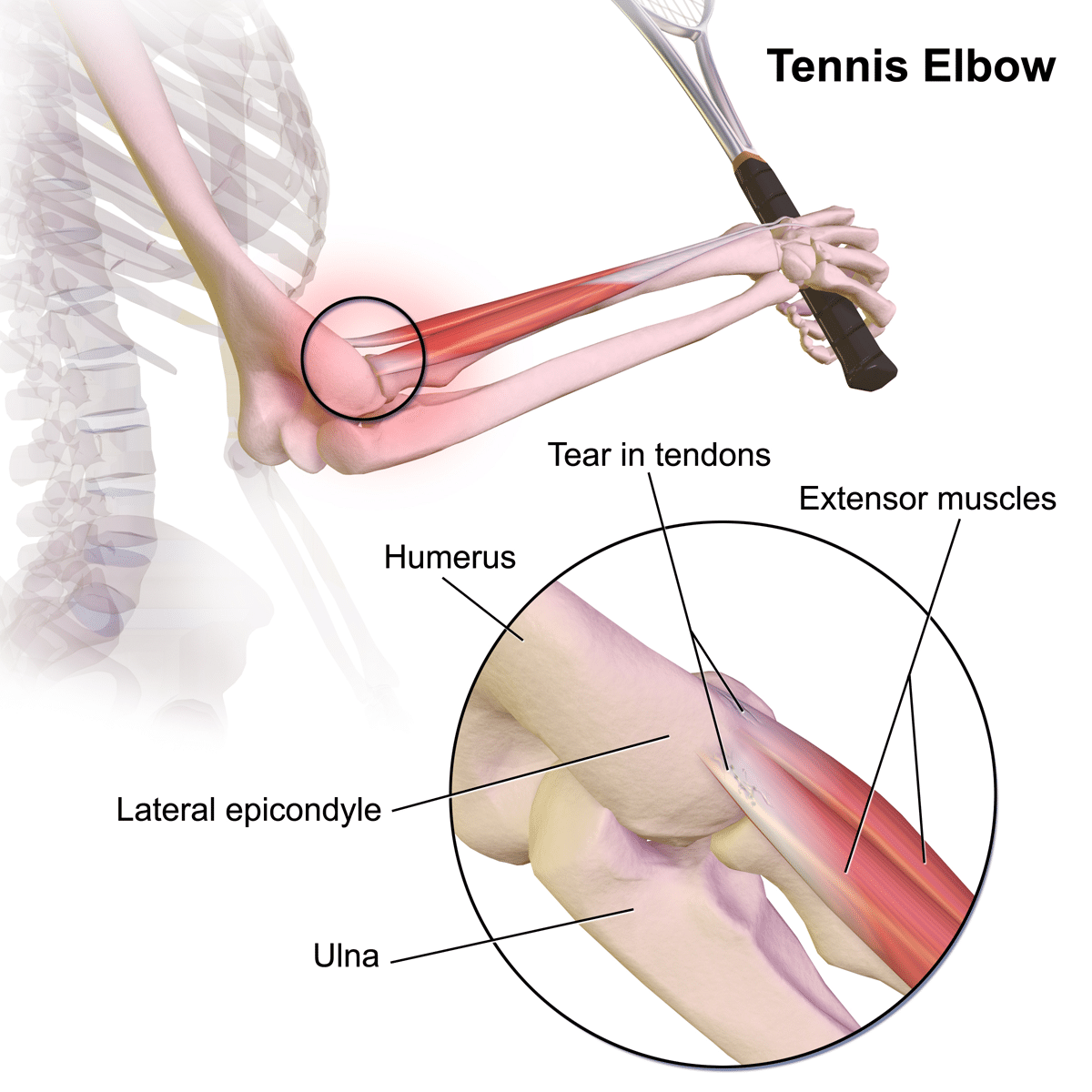
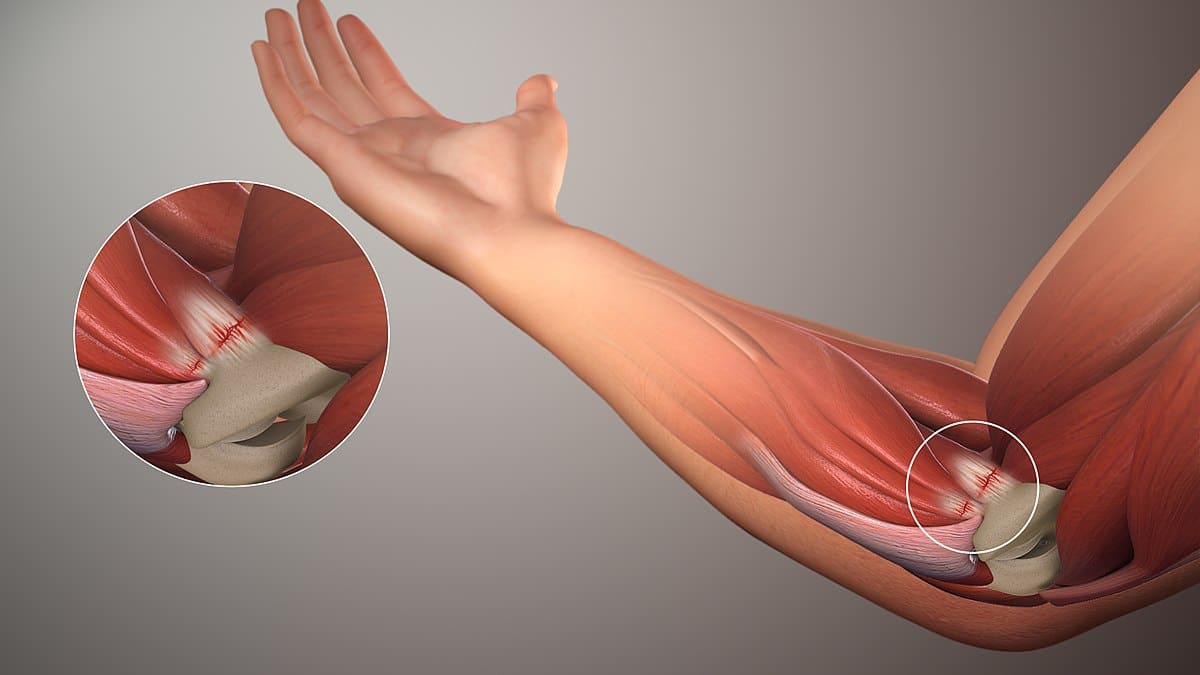
Occupational data from the general population indicates that the risk of experiencing golfer’s elbow and tennis elbow is significantly elevated for people who repetitively perform forceful activities involving the elbow, forearm, and wrist (47,48,58,182,205). To my knowledge, no study has yet to investigate how different resistance training program variables may affect a lifter’s risk of developing golfer’s elbow or tennis elbow. Correspondingly, I won’t be making any definitive claims as to how programming decisions will increase or decrease your risk of experiencing these injuries, nor will I be providing medical advice. However, I have two general recommendations based on the evidence available about tendinopathies and injuries more broadly and what we know about golfer’s elbow and tennis elbow specifically.
The first recommendation is to use a gradual volume progression if you wish to add some of the exercise variations discussed throughout this article into your program with the intent of improving grip strength and forearm muscle size. Along with many lifts that you may already be performing, all of those grip exercises will provide a training stressor to the common flexor tendon and/or common extensor tendon. With repeated exposure to stress, tendons can adapt over time to progressive loading, but a sudden spike in loading to which they are unaccustomed may increase the risk that the stress exceeds their capacity (100). People who prioritize enhancing grip strength may particularly find that it is easy to overuse hand grippers due to their convenience and minimal systemic fatigue. These qualities make them valuable tools for increasing total training volume, but be careful to not be excessive with how many sets you perform each week.
Secondly, if you begin to notice clear symptoms of either golfer’s elbow or tennis elbow, I recommend not simply to push through it without making any modifications to your training. If you are passionate about lifting and committed to achieving your goals, it may be quite tempting to do so, particularly because a tendinopathy may initially manifest as only a mild pain that does not prevent you from having productive training sessions early on. What may begin as a minor nuisance that can be ignored with some NSAIDs and ice can snowball into a serious impediment as weeks and then months pass by without the appropriate behavioral changes.
I expect that essentially everyone who has been consistently training for years at the very least has experienced a mild ache or discomfort near a joint that differs from muscle soreness. Pain is a complex phenomenon, and having a minor ache that develops shortly after a challenging workout does not necessarily mean that an injury occurred and you should panic. For instance, I’m sure that plenty of powerlifters have had a bit of low back discomfort (that differs from spinal erector muscle soreness) at some point in their lives a day or two after a tough deadlift and squat session. These sensations may occur in the absence of actual tissue damage and resolve in a short period of time. Having a transient bout of mild low back pain every now and then does not mean that a disc herniated in the same way that having a bit of medial epicondyle discomfort for a day does not mean that the common flexor tendon is injured. However, pain continuing to persist in a particular area and consistently be aggravated by certain types of activities is a warning sign that something may be amiss and worth addressing. With respect to golfer’s elbow and tennis elbow, the hallmark feature of which to be aware is pain and tenderness near the elbow that is aggravated by gripping activities (84). For golfer’s elbow, pain and tenderness are localized to the medial epicondyle, while they are localized to the lateral epicondyle for tennis elbow. Because loading the involved tendons can provoke pain from tendinopathy, resisted wrist flexion and/or forearm pronation may be painful with golfer’s elbow (84). On the other hand, resisted finger extension and/or wrist extension may be painful with tennis elbow depending on which tendon sites are affected (91). Testing whether these resisted movements are provocative is a key component of physical exams that physical therapists utilize when assessing patients who are suspected of having tennis elbow or golfer’s elbow prior to designing their treatment plans. If either condition becomes chronic, elbow pain may also be accompanied by weakness in wrist certain movements and grip strength deficits (51,157,158,167).
Since I am not providing any medical advice and do not intend for my recommendation to be misconstrued as such, I will briefly explain some of what I would do if I developed symptoms of golfer’s elbow or tennis elbow. Previously I dealt with a hamstring tendinopathy from running cross country in high school that became chronic after pushing through it and then patellar tendinopathy from jump training that took over a year and a half to resolve because of short-sighted decision making on my part. A couple years ago, I also developed golfer’s elbow from resistance training after a block of heavy weighted pullups and chinups. However, I was able to resolve this tendinopathy in a much briefer period of time after applying what I learned from the prior injuries and extensive reading into tendinopathy research and clinical practice.
If I noticed new symptoms of golfer’s elbow or tennis elbow in my quest to increase grip strength, the first thing I would do is temporarily reduce my volume of grip training and refrain from the particularly aggravating activities. For instance, if hand grippers, pull ups, and heavy mixed grip deadlifts were the most provocative activities, I may substitute in lighter cable pulldowns with very strict technique for pull ups, perform heavy deadlifts with straps, and take a break from hand grippers all together. The volume required to maintain strength is lower than what is required to increase strength, so grip strength should not meaningfully decrease if a couple weeks of training are performed with one third of prior grip training volume (22).
While reducing the volume of the particularly stressful activities, I would regularly perform low velocity (e.g., three-second concentric phase and three-second eccentric phase) forearm exercises that directly load the tendons originating at the painful site. For instance, I would likely utilize wrist flexion, radial deviation, and forearm pronation exercises to manage golfer’s elbow. On the other hand, I would likely use wrist extension, radial deviation, forearm supination, and finger extension exercises to manage tennis elbow. Repeated loading in excess of the tendon’s load tolerance is what contributes to the development of tendinopathy in the first place, but properly applied loading is also a key component of tendinopathy rehab due to its ability to increase a tendon’s load tolerance. As with patellar and Achilles tendinopathies, the available body of evidence indicates that resistance training interventions can serve as viable treatments for tennis elbow (34,42,44,92,113,135,150,160,188,189). The majority of resistance training interventions assessed for their potential to treat tendinopathies have been eccentric only in nature, but there is no evidence indicating that conventional concentric-eccentric resistance training would be any less effective (21,43,100,189). For tendinopathy treatment, eccentric-only exercise is likely superior to concentric only exercise, but interventions composed of both concentric and eccentric actions have been similarly effective to eccentric only programs (21,85,100,155,189). Golfer’s elbow is considerably less common than tennis elbow (even among golfers ironically), and this discrepancy is reflected in the volume of research that investigates treatment for these two conditions (84,124,181). In addition to a case series that lacks any control group, I was only able to find a single randomized trial assessing the potential of an exercise intervention to treat golfer’s elbow, and it lasted only four weeks with 15 participants in the exercise group (5,193). Consequently, there is a notable gap in the current body of literature, but it is quite plausible that golfer’s elbow could respond in a manner similar to other tendinopathies in response to resistance training.
Mixed Grip Deadlifts & Biceps Tendon Ruptures
Multiple studies have examined how deadlifting with straps may differ from doing so without straps, but the research has concentrated on usage of the double overhand grip when pulling without straps (41,61,86,87,88,89,198). For non-powerlifters who wish to deadlift to increase strength and muscularity in the posterior chain, exclusively using straps for work sets is a completely viable approach, especially if other exercises are used to directly train the forearms. When opting to not use straps, some lifters may only deadlift with a double overhand grip, but it can severely limit the weight experienced lifters can pull. To reduce the likelihood of the bar rolling out of their hands, the mixed grip or hook grip may alternatively be used. Of these two options, recreational and competitive lifters alike commonly use the mixed grip (AKA alternate grip), where one forearm is pronated while the other is supinated. The mixed grip requires some training experience to adapt to using it, but the time needed to develop proficiency while pulling with it is considerably less than the hook grip, which can feel very uncomfortable on a lifter’s thumbs (202). However, some individuals are concerned about the potential to develop muscle imbalances as a result of consistently pulling with a mixed grip. This may prompt some people to alternate which side is supinated from set to set, but I doubt that practice is worthwhile for most lifters.
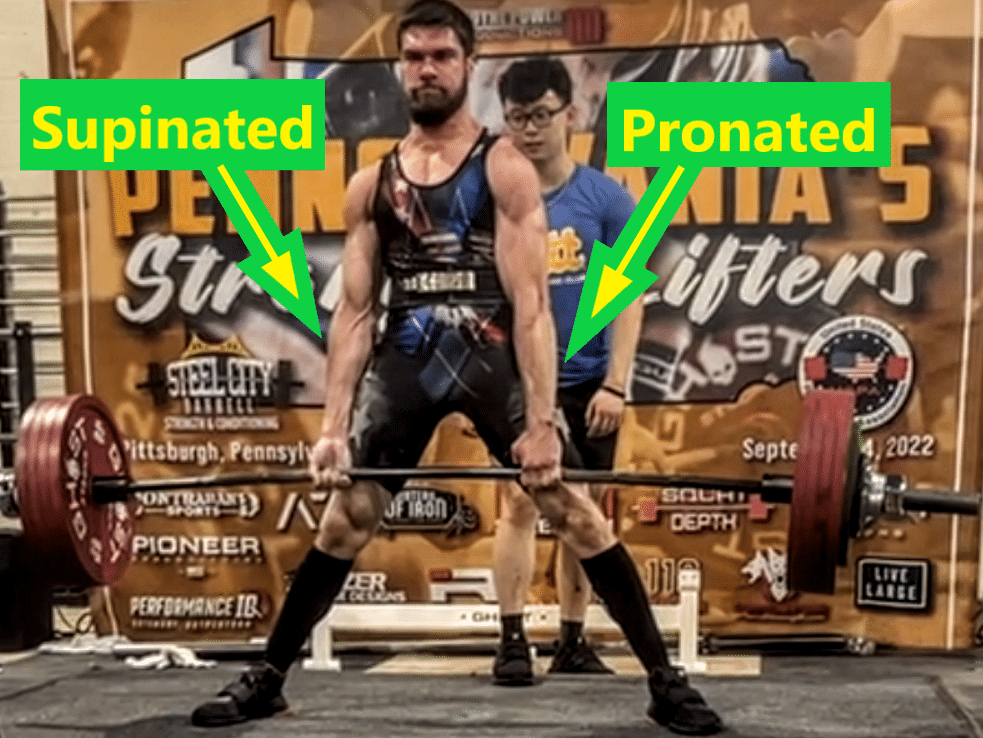
To my knowledge, only one study has compared muscle activation between mixed grip deadlifts and double overhand deadlifts (19). Beggs (2011) assessed 10 trained participants with an average conventional deadlift 1RM of 202.5kg (446.4lb) as they performed 3 sets of 2 reps with 60% 1RM and 80% 1RM. When initially testing their deadlift 1RMs, participants were free to use straps or whichever grip they preferred. Given the major limitations of the double overhand grip for trained lifters, participants were also free to use straps during the double overhand grip trials at 80% 1-RM, which they all opted to use. However, straps were explicitly prohibited when deadlifting 60% 1RM. As the participants deadlifted, Beggs measured the EMG activity of the right and left biceps, brachioradialis, upper trap, and upper lat. Deadlifting with a mixed grip yielded significantly greater EMG activity of the biceps on the supinated side compared to the pronated side of the mixed grip trials or either biceps in the double overhand and straps conditions. Average brachioradialis activation also exhibited a trend of lower activation on the supinated side relative to the pronated side during mixed grip deadlifts. However, upper trap and upper lat EMG activity were similar regardless of the grip used for deadlifting. Asymmetrical activation of other muscle groups or muscle regions not measured potentially may be present during mixed grip deadlifts. Nonetheless, the net effect on overall side to side differences in muscle size and strength may still be insignificant when mixed grip deadlifts are included in a program that trains these muscles symmetrically with other exercises. More of a hazard than developing any potential mild asymmetry is the elevated risk of sustaining a distal biceps tendon rupture imparted from a mixed grip.
While rare in the general population, the distal biceps tendon of the supinated arm is more susceptible to rupture in males who deadlift (90,95). Empirical data on the matter is unavailable, but I expect that the risk of this rupture would be elevated if a deadlift is initiated with slight elbow flexion on the supinated side in a “grip and rip” style. Doing so could result in that elbow rapidly extending under a very heavy load, imparting considerable eccentric loading into a stretched distal biceps tendon. In addition to mixed grip deadlifts, distal biceps tendon ruptures have also been recorded to occur during biceps curl variations and strongman events such as the tire flip and atlas stone lift. While I will not make any definitive claims, distal biceps tendon ruptures potentially may be more likely to occur during a free weight preacher curl relative to other curls due to its strength curve. When gravitational force is providing resistance during a free weight curl, resistive torque peaks when the horizontal distance between the weight and elbow joint is greatest, which occurs when the forearm is perpendicular to the ground. During a standard curl with your upper arms held near your sides (i.e., having close to about 0° of shoulder flexion), your forearms will be horizontal to the ground when your elbows flex to about 90°. In contrast, your elbows will be in lower angles of flexion when your forearms are horizontal to the ground during preacher curls due to the flexed shoulder position. This results in resistive torque peaking at longer muscle lengths for the biceps during free weight preacher curls compared to standard free weight curls or curls performed with cables or machines that provide an even level of resistance throughout the ROM. The degree to which the biceps are lengthened when resistive torque peaks during a free weight preacher curl will vary depending upon the slope of the preacher curl pad and the seat position a lifter selects. In addition to using a pad that is more horizontally inclined, utilizing a lower seat height or sitting further back can contribute to a more flexed shoulder position that shifts peak resistive torque to more extended elbow angles. Based on footage, if a distal biceps tendon ruptures during a preacher curl, it appears to be most likely near the end of the eccentric phase when the elbow is in a low angle of flexion and the tendon is loaded in a fairly lengthened position.

For lifters who intend to perform free weight preacher curls, I generally recommend that they select moderately light loads (i.e., enabling at least 12 reps per set) that they can control through a full ROM with a slow eccentric phase. Some lifters intentionally avoid the more extended elbow angles during preacher curls by performing partial ROM reps with weights that are too heavy to control through a full ROM. The concern with that approach would be if a lifter unintentionally moves into more extended elbow angles with a weight that exceeds what someone could move concentrically from extended joint angles. If this occurs, the biceps tendon would be subjected to supramaximal eccentric loading in a stretched position which is not trained by flexed elbow partial ROM curls. As with other injuries, an abrupt spike in training volume also has the potential to increase someone’s likelihood of a tendon injury (29,30,50,79,118,140). Consequently, a gradual workload progression is prudent for exercises that impart high loading to the biceps tendon in a stretched position just as it is wise when incorporating gripping exercises that we previously discussed.
Conclusion
If you prioritize strengthening a particular type of grip, such as a mixed grip or hook grip for the deadlift, the accessory exercises discussed in this article can be valuable tools to utilize alongside higher specificity training. Once you have adapted to using a specific grip, you do not need to train that exact grip with a high frequency approach to progress. Gripping something heavy is not a technically complex maneuver, but a minimum frequency of exposure to a specific type of grip is still important to ensuring that more general training is able to transfer effectively. Performing a high volume of general grip training for a few months can increase your potential deadlift strength with a mixed grip or hook grip, but these grips can feel quite awkward if you refrain from training them for too long. Even if you opt to not train with these specific grips intensely on a frequent basis, I recommend utilizing them with a least some degree of regularity for submaximal training, such as light speed pulls. As with any other facet of training to enhance performance, some trial and error may be required to determine what level of specificity is optimal for you as an individual. While much knowledge can be gained by exploring the available body of empirical evidence, training is both an art and a science. A variety of means can be used to reach certain goals such as increasing grip strength and forearm muscle size. Through this article, I hope that you are now better equipped to utilize these different approaches in pursuance of your own individual goals.
Whether you strive to increase grip strength or develop a more muscular looking physique, direct training of the forearm muscles can be a beneficial component of your program. While other muscles play a role, no two are more impactful to either pursuit than the flexor digitorum superficialis and flexor digitorum profundus, which flex the finger joints and the wrist. Training these powerful muscles along with other muscles in the forearm and hand can help improve long-term grip strength and forearm muscle size simultaneously.
Summaries
As you can readily see, this article is quite lengthy and really delves into the details that can help you draw your own conclusions and apply the available body of evidence to your own unique situation. Due to this length, having some concise summaries about the key points for each training method can also be useful.
Extremely high specificity support grip training (e.g., training heavy mixed grip deadlifts to increase mixed grip strength for the deadlift)
Pros:
- Most effective for inducing neural adaptations that have greatest immediate transfer to the specific grip strength
- May help increases in muscle size stimulated by other exercises transfer to greater performance with that specific grip
- Can increase confidence when executing that specific exercise
- Facilitates improvements in technique for that specific exercise
- May increase the load tolerance of certain tissues in a manner difficult to replicate with other exercises
Cons:
- Training volumes may be limited by other factors besides recovery of forearm and hand muscles (e.g., lumbar structures due to high axial loading, hand skin due to knurling)
- Likely suboptimal for stimulating forearm and hand muscle hypertrophy and therefore unlikely to maximize long-term grip strength potential when used exclusively
- May be more globally fatiguing than other exercises
- Requires equipment that may only be available to you in a gym
Similarities among training with hand grippers, fat grips, and dynamic wrist exercises
Shared pros:
- Likely more effective in stimulating forearm and hand muscle hypertrophy than typical support grip exercises, which can increase long-term strength potential for various grips
- Volumes unlikely to be limited by recovery of muscles other than those in the forearm and hand
- May impart lower global fatigue than very high specificity training
- Unlikely to tear a callus
- Can be used to train grip strength if an injury precludes high specificity training
Shared con:
- Suboptimal for inducing neural adaptations specific to a different type of grip, so transfer to a different type of grip may be limited if additional exercises are not performed while using that specific grip
Hand gripper training distinct pro
- Extremely convenient in the sense that it can be performed nearly anywhere
Fat grip training distinct pro
- Can be very time efficient when fat grips are added to exercises you already perform
Dynamic wrist exercises distinct pro
- Likely the most effective method of increasing forearm muscle size
Sample Training Programs
Optimal results typically require individualized plans, but sample training programs for different goals can also help provide a solid starting point as to how this info can be applied in a manner that will be beneficial for many people. If you opt to utilize one of the sample programs as a template, I recommend progressively building up to the volumes they include over the course of multiple weeks. For instance, you can begin with two sets of a particular exercise in the first week and add one or two sets each week until you reach the number of weekly sets you wish to consistently perform. Once you have acclimated to performing the set volumes in the sample programs for a handful of weeks, you can gradually increase the volume if you have more time available to train and wish to increase your rate of progress. In the sample programs, you will notice hand gripper exercises and fat grip exercises are not included. I did not specifically program them because I generally recommend performing them when they are most convenient to you as a means of accumulating greater forearm training volumes without investing further time training. Additionally, some people do not own hand grippers or fat grip attachments, and they typically are not available in a commercial gym.
Goal: Increase forearm muscle size in a time-efficient manner
Finger flexion wrist curls: 2-3 sets of 12-20 reps 2x/week
- Can use dumbbells or barbell
Wrist extensions: 2-3 sets of 12-20 reps 2x/week
- Can use dumbbells or barbell
Your elbow flexion curl of choice: 2-3 sets of 8-15 reps 2x/week
- Can use whatever equipment you prefer
Details: Depending on your available equipment and preference, you can perform either exercise bilaterally or unilaterally. Perform the two wrist exercises as a superset, and execute as many reps as possible until muscular fatigue for each set. Consistently performing 4-6 quality sets of each exercise per week is likely sufficient to stimulate increases in forearm muscle size if you have not already been utilizing these exercises. However, progressing to greater volumes, such as 4-5 sets of each exercise per session, may yield better results for more experienced lifters. Distributing the same weekly training volume into three sessions per week (e.g., performing 2 sets 3x/week instead of 3 sets 2x/week) can also be similarly effective. With either frequency, I recommend spacing your training sessions evenly throughout the week, such as performing these exercises on Monday and Thursday with a 2x/week approach or Monday, Wednesday, Friday with a 3x/week approach.
Where specifically in your pre-existing training program that these exercises are most beneficial to incorporate will be influenced by the rest of your training, but the chief goal is that you place them in a position that does not noticeably detract from your performance of other exercises. Acutely after performing the wrist exercises, the resulting fatigue in your forearm and hand muscles will reduce your grip force, so you should keep that in mind while deciding where to perform them within a particular training session and within a training week. So long as you perform them at a time that does not interfere with other training goals, these exercises can be added into a lower body or upper body focused training session or even an “active recovery day” where you refrain from more strenuous resistance exercises.
Goal: Increase barbell specific support grip strength for the deadlift
Suitcase rack pull hold: 2 sets of 20-40s 2x/week
- Select a load that causes your grip to approach failure after about 20-40 seconds
Dead hang: 2 sets of 20-40s 2x/week
- Depending on your strength level, you can perform this unilaterally or bilaterally and with or without resistance added to your bodyweight. Select a variation that causes your grip to approach failure after about 20-40 seconds of hanging.
Finger flexion wrist curls: 2-3 sets of 12-20 reps 2x/week
- Can use dumbbells or barbell
Wrist extensions: 2-3 sets of 12-20 reps 2x/week
- Can use dumbbells or barbell
Details: I recommend performing these exercises in addition to using your mixed grip or hook grip for the deadlift to experience the greatest carryover. The specific programming variables for the deadlift itself are not included in this sample because the focus of this article is on grip strength, and considerable variation exists with how different individuals program deadlifts. The key is that you are utilizing the specific grip you wish to strengthen for your deadlift on a somewhat regular basis rather than exclusively relying on straps. For instance, you may use your mixed grip for warm-up sets and one top deadlift set in a session while using straps for other sets if your grip strength would limit performance in those sets. To develop your support grip strength further at finger joint angles specific to those used when deadlifting, you can perform the suitcase rack pull hold and dead hang after your deadlifts. If you only deadlift once per week and prioritize increasing your grip strength for the deadlift, you can additionally perform the suitcase rack pull hold and dead hang on another training day that is 3-4 days after your deadlift day. For instance, if you deadlift on Monday and squat on Thursday, you can perform the suitcase rack pull hold after your squat sets on Thursday. Either at the end of those sessions or during the day afterwards, you can perform the finger flexion wrist curls and wrist extensions as a super set. Given the value of increasing muscle size for improving long-term strength potential, all of the programming details previously discussed about these exercises can apply to their incorporation into a plan that focuses on enhancing support grip strength.
Goal: Optimize increases in forearm muscle mass and/or increase strength in each wrist movement for a specific activity (e.g., arm wrestling)
Finger flexion wrist curls: 4-5 sets of 12-20 reps 2x/week
- Can use dumbbells or barbell
Wrist extensions: 4-5 sets of 12-20 reps 2x/week
- Can use dumbbells or barbell
Forearm pronation and supination: 2 sets of 12-20 reps 2x/week
- Can use asymmetrical weight
Radial deviation: 2 sets of 12-20 reps 2x/week
- Can use asymmetrical weight or band
Ulnar deviation: 2 sets of 12-20 reps 2x/week
- Can use asymmetrical weight or band
Your elbow flexion curl of choice: 4-5 sets of 8-15 reps 2x/week
- Can use whatever equipment you prefer
Details: This approach is chasing diminishing returns and not required for most people to increase forearm muscularity or strength in various wrist movements. However, the additional time investment can be worthwhile for certain individuals, and personal goals are unique to each individual.
Extra Info
While preparing to write this article, I looked over hundreds of different research articles related to grip strength and the forearm muscles. Some of these did not provide information directly relevant to the specific topics covered throughout the article but can be interesting in their own right even if they confirm what may be presumed as common knowledge. For those who are curious to learn more, this section briefly summarizes the findings from some of those articles.
On average, untrained individuals have greater forearm muscle volume in their dominant side than their non-dominant side, and this forearm asymmetry is significantly greater in tennis players and fencers (120,123,169,170). The magnitude of difference meaningfully varies depending upon the source, but people generally have greater grip strength in their dominant hand (e.g., right hand for right-handed people) compared to their non-dominant hand (15,25). Based on the available data, about a 5% difference in grip strength between hands appears to be normal in the general population. Using MRI, Sanchis-Moysi et al (2010) assessed the volumes of different forearm muscle groups in pro tennis players and found the superficial flexors, deep flexors, and extensors to be 12.3%, 7.6%, and 5.7% more voluminous in the forearm of their dominant arms compared to non-dominant arms (169). Cross-sectional research limits us from concluding that a causal relationship exists, but these findings suggest that high volume submaximal loading of the forearm muscles can be hypertrophic to at least some degree. On average, grip strength is greater when tested in a standing position compared to a seated position, and it is also typically greater when tested with an extended elbow position compared to a flexed elbow position (13,56,104,122,148,152,191,212).
Trossman and Li (1989) assessed untrained participants as they performed maximal isometric crush grip tests 15 seconds, 30s, or 60s after an initial grip test to determine how rest intervals influence grip strength fatigue (199). Relative to the initial grip test performed in an unfatigued state, grip strength was on average 12%, 10%, and 7% lower respectively after 15s, 30s, and 60s rest intervals. Finger flexion strength and forearm circumference exhibit significant positive correlations with rock climbing performance (185). Advanced class climbers have significantly greater average finger flexion strength and forearm circumference than intermediate class climbers, who themselves have significantly greater average finger flexion strength and forearm circumference than novice class climbers. Low load dynamic crush grip exercise acutely results in greater increases in hand and wrist volume than static crush grip exercise with the same load, indicating that dynamic grip exercise may result in a greater “pump” to the working muscles (214). Compared to having a bare hand, wearing gloves can reduce maximal grip force, particularly when wearing thicker gloves (101,207). Grip strength has been measured to be similar acutely after untrained participants inhale ammonia salts or water (the control) (35). This lack of transient strength enhancement following ammonia salt inhalation is congruent with research using other strength tests (e.g., deadlift 1RM and squat/bench press reps to failure with 85% 1RM) as covered by Hayden Pritchard on Stronger By Science. For female powerlifters, grip strength exhibits moderate strength positive correlations with deadlift 1RM, squat 1RM, and powerlifting total (192). In young untrained women, grip strength exhibits a statistically significant, albeit small magnitude, positive correlation with serum Vitamin D levels (80). In a landmark study, Ozerkan (2001) found participants to demonstrate greater grip strength directly after looking at a drawing of a “smiling face” compared to a drawing of a “crying face” (149).
Forearm Muscle Primary Function Chart
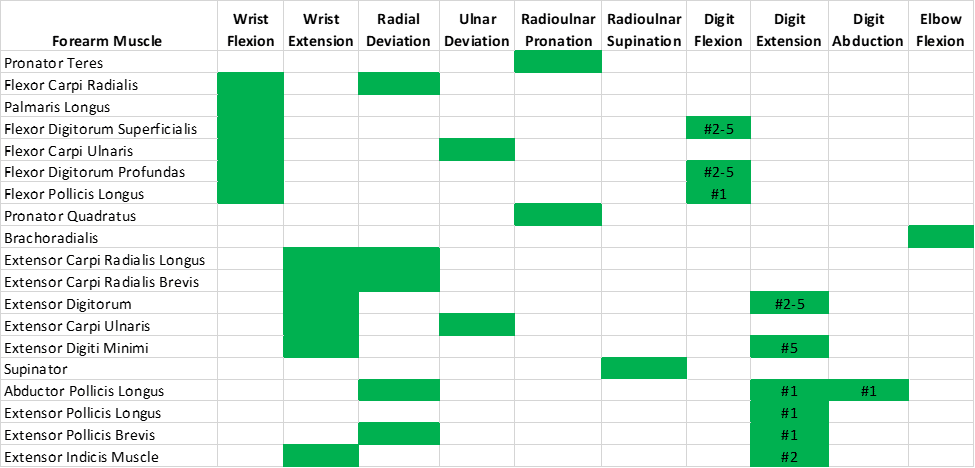
I made this chart as a visual summary of the primary joint functions of 19 forearm muscles (excluding the anconeus because it lacks a primary dynamic function) based on the available biomechanical data (62,63,69,153,162). Boxes shaded in green indicate the primary functions for the corresponding muscles. For the digit functions, #1 corresponds to the thumb, #2 corresponds to the index finger, #3 corresponds to the middle finger, #4 corresponds to the ring finger, and #5 corresponds to the little finger. Note that this chart does not display secondary functions to which a muscle may contribute such as elbow flexion for the extensor carpi radialis longus. While the muscles may be able to assist in generating torque during multiple other movements not shaded in green, they will be trained meaningfully better with exercises that resist their primary functions. For certain muscles, universal agreement exists with respect to having a primary function, such as the pronator teres functioning as a primary forearm pronator. However, discrepancies exist across different articles and textbooks in terms of which primary functions are assigned to various muscles. I believe that these discrepancies arise in large part due to an absence of an objective method to classify primary muscle functions. To account for these differences, I developed objective criteria to classify primary muscle functions for the table based on quantifiable data. As is often the case when selecting numerical thresholds for classifications, the precise cut-off values are somewhat arbitrary, and I am by no means asserting that the values I chose are the only valid ones that can be used. However, I am under the impression that the criteria I developed result in functional classifications that are congruent with those where consensus exists while removing subjectivity from inconsistent classifications.
Provided that a muscle’s anatomical attachments allow the force generated by its contraction to contribute to generating a moment at the joint, a muscle can be classified as a primary contributor to a particular joint function if:
A) Its peak moment arm for that joint function is greater than 50% of the muscle with the greatest peak moment arm for that joint function.
OR
B) Its potential peak moment (peak moment arm X physiological cross-sectional area) for that joint function is greater than 50% of the muscle with the greatest potential peak moment for that joint function.
Sources
The hand skeletal anatomy, forearm skeletal anatomy, hand joint anatomy, intrinsic hand muscle anatomy, forearm muscle anatomy, length tension relationship, superficial forearm muscle anatomy, and deep forearm muscle anatomy images were published by “OpenStax,” are licensed as a Creative Commons work, and can be found here.
The fingertip grip deadlift image of David Woolson was published by Brazos Valley Barbell’s YouTube channel and can be found here.
The Tom Cruise fingertip grip image was a screenshot from Mission: Impossible 2, which was released by Paramount Pictures in 2000 and can be found here.
The Jamar® Hydraulic Hand Dynamometer image was published as a product picture by Global Industrial and can be found here.
The CAMRY Digital Hand Dynamometer image was published as a product picture by Amazon and can be found here.
The flexor digitorum superficialis, flexor digitorum profundus, and flexor pollicis longus muscle anatomy image was developed with 3D4Medical’s Complete Anatomy for an educational publication as permitted by my student license.
The Devon Larratt image was produced by Jerry Milne and can be found here.
The IronMind pinch grip block image was published as a product image by Grip & Lift Australia and can be found here.
The grip strength testing and wrist extension training images were developed by Shimose et al (2011) as Figure 2 and Figure 3 from Effect of submaximal isometric wrist extension training on grip strength, which was published in the European Journal of Applied Physiology, and can be found here.
The wrist extension exercise image from figure 1 from Souza et al (2017) can be found here in their article published by Fisioterapia e Pesquisa.
The finger flexion training and testing images from figure 1 from Shim et al (2008) can be found here in their article published in Motor Control.
The squeeze ball, hand gripper, and dynamometer image from photograph 1 from Sharma et al (2020) can be found here in their article published by Indian Journal of Public Health Research & Development.
The humerus epicondyle anatomy image was published by Doctor Jana, is licensed as a Creative Commons work, and can be found here.
The tennis elbow image was published by Bruce Blaus on Wikimedia Commons, is licensed as a Creative Commons work, and can be found here.
The golfer’s elbow image was published by Scientific Animations, is licensed as a Creative Commons work, and can be found here.


