

We’ve all experienced the agony. The pain of trying to get out of your car, wobble up the stairs, or move normally after a hard workout. This soreness is called delayed onset muscle soreness (DOMS). If you’ve been exercising long enough, you’ve probably felt it. Some lifters relish this pain as an indicator of success, but is that really the case?
What is DOMS?
I frequently see DOMS occur after a daunting leg day. It can also occur in experienced lifters after taking a few weeks off. Studies show (1) that it’s not restricted to any particular muscle group, but some people tend to experience it more in certain muscles.
Technically speaking, DOMS is (primarily) caused by a type 1 muscle strain – some degree of fiber damage, but nothing too serious – predominantly as a result of unaccustomed exercise. As you may have experienced, DOMS can range from slight muscle discomfort to severe pain that limits range of motion. Generally, muscle soreness becomes noticeable ~8 hours post-workout and peaks 48-72 hours later, although the exact time course can vary.
There is little doubt that DOMS is correlated with exercise-induced muscle damage to some degree; however, measures of muscle damage at a microscopic level are poorly correlated with reports of soreness. Basically, if you’re really sore, it doesn’t mean you completely “shredded” your muscles. This is supported by MRI images showing little damage to some muscles post-exercise. Not only do the time course of changes in the markers of muscle damage differ from one another, but they also don’t match the time course of muscle soreness (Newham, 1988). It is possible for severe DOMS to develop with little or no indication of muscle damage, and for severe damage to occur without DOMS.
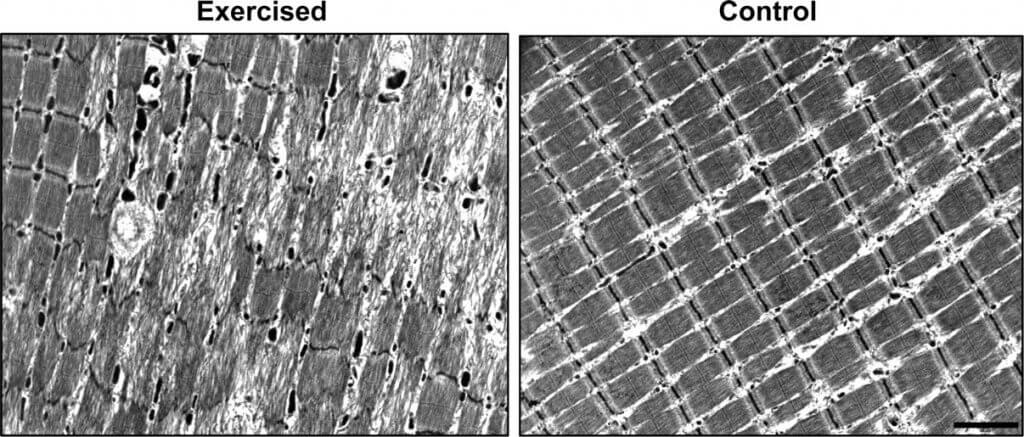
Certain types of exercise can cause significant muscle damage. The image below is taken after an extensive eccentric exercise protocol. As you can see, the muscle fiber just looks messed up. The majority of studies examining exercise-induced muscle injury and DOMS use untrained subjects undertaking large amounts of unfamiliar eccentric exercise. This model is unlikely to closely reflect the circumstances of most people who workout. However, it does give us some insight into what happens in the muscle.
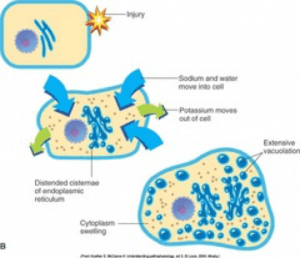
Another DOMS-inducing stimulus that occurs during exercise is metabolic stress (and I’m not talking about the build-up of lactic acid, which does not cause DOMS. Thinking that lactic acid causes muscle soreness is a dogmatic idea that is thoroughly outdated and flat-out wrong). After high-intensity exercise, rest alone will return blood lactate to baseline levels well within the normal time period between training sessions. However, there is some evidence that hydrogen ions and reactive oxygen species – both of which increase in concentration during exercise – may contribute to DOMS (2). Metabolic stress during exercise can cause changes on a structural level at the cell membrane (sarcolemma). The damage allows fluids and other factors to enter the cell, which promotes inflammation (3).
Does DOMS mean more muscle growth?
Some studies show the presence of DOMS after long-distance running, which indicates it doesn’t just occur during resistance training. This should be an anecdotal indicator that DOMS isn’t a good gauge of muscle growth since running causes minimal hypertrophy.
People who are new to working out often have the most pronounced DOMS. They also happen to grow the most, so you can see how the two may be intertwined. This is due to the new stimulus that exercise provides. Again, they get sore because they aren’t accustomed to exercising – not because they are growing like monsters. Interestingly, there is no difference in DOMS between sexes even for beginners (4).
There is some evidence to show DOMS may negatively affect workouts by altering motor patterns in subsequent workouts. This could cause reduced activation of the desired muscle (5). Hence, DOMS could actually hinder your next workout. In addition, severe DOMS can decrease force capacity by up to 50% (6). This causes functional deficits that may impair training at a certain level, which could hinder muscle growth in the long term.
Exercising while having DOMS does not seem to make muscle damage worse (7), but it may interfere with the recovery process. In extreme cases, exercise-induced muscle damage can cause rhabdomyolysis, a serious condition that can lead to renal failure. So be careful when throwing a newbie into an advanced program – especially if they’ve never exercised. You could do some serious damage.
How do I feel DOMS?
So if you aren’t destroying your muscles or burning them up with lactic acid, then why do they hurt? I recently discussed this concept with a member of my lab.
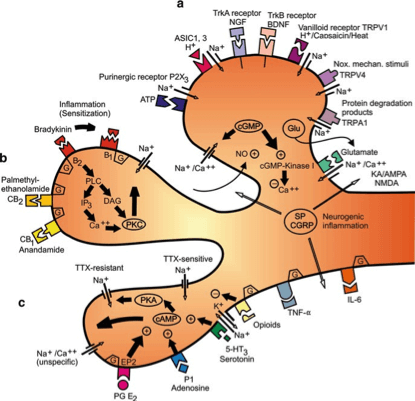
Nociceptors are free nerve endings that respond to damaging stimuli by sending pain signals to the brain. In muscle tissue, these receptors can sense chemical stimuli such as inflammation or disturbances in microcirculation to blood vessels. These receptors are not inside the muscle because muscle cell death is not painful. In comparison, tearing a muscle can be extremely painful. The pain is due to the release of muscle substrates into the space where nociceptors are located. This also helps us appreciate that DOMS probably doesn’t occur due to something inside the muscle (i.e., in the contractile apparatus) (7).
How can I reduce DOMS?
One of the best ways to decrease the risk of DOMS is to slowly progress into a new exercise program. If you’ve ever had an advanced program, you’ll notice the first week or two may have reduced volume. The “prep” phase of programs has two purposes: 1) allowing the muscle time to acclimate to a new movement, and 2) leaving room for more adaptation.
We all know we should warm-up properly. This is probably one of the only times you’ll hear it doesn’t help. While it may prepare you for exercise (I highly suggest it), neither warming up nor stretching before exercise has been shown to reduce or prevent DOMS.
Something a lot of people use to relieve DOMS is foam rolling. However, it has only been shown to improve DOMS in some studies. During foam rolling, you use your own body mass on a foam roller to exert pressure on an area of soft tissue. The motion places direct pressure on an area, which stretches it. It is considered self-induced massage because the pressure somewhat resembles the pressure exerted on muscles by a massage therapist. Again, there are only a few studies that have measured the effects of foam rolling on performance. These studies found foam rolling can enhance recovery after DOMS and alleviate muscle tenderness. Self-massage through foam rolling could benefit people wanting to recover in an affordable, easy, and time-efficient way.
Another intervention commonly used is massage. Some researchers have shown decreases in pain associated with DOMS after a massage (8). However, massage has no effect on muscle metabolites such as glycogen or lactate. One study found massage decreased the production of the inflammatory cytokines by mitigating cellular stress resulting from muscle injury (8). Many people believe massage can provide increased blood flow to specific areas, reduced muscle tension, and mood enhancement. Massage produces direct pressure, which may increase ROM and decrease stiffness. These benefits are expected to help athletes by enhancing performance and reducing injury risk. The effects of timing of massage (pre- or post-exercise) on performance, injury recovery, or injury prevention are not clear because the mechanisms of each massage technique have not been widely studied.
Supplements to reduce DOMS
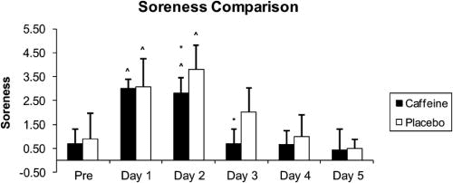 Caffeine has long been known to increase alertness and endurance, shown by the the average person’s morning grumpiness before drinking the black gold. Interestingly, a recent study by Hurley et al., reported caffeine has the ability to reduce DOMS. They mesured perceived soreness in males consuming caffeine one hour before a workout. They found a lower level of soreness in the biceps on day 2 and 3 compared to a placebo after subjects completed a bicep curl protocol. Using a dosage of 5mg/kg bodyweight they found a beneficial effect of caffeine on soreness. For comparison, a 185lb (~84kg) male would take about 420mg of caffeine preworkout. That is a ton of caffeine! An 8oz Red Bull contains roughly 85mg. Does your preworkout supplement have that much caffeine? Probably not. If you’re wondering when caffeine peaks in the blood, it’s about one-hour post ingestion. Caffeine is an adenosine antagonist and affects the activity of central nervous system (CNS) by blocking adenosine receptors, thus resulting in decreased levels of soreness. This suggests that short-term caffeine ingestion before a strenuous workout may decrease overall soreness levels. However, the subjects who took caffeine were able to perform more reps than the control group, which could be a confounder.
Caffeine has long been known to increase alertness and endurance, shown by the the average person’s morning grumpiness before drinking the black gold. Interestingly, a recent study by Hurley et al., reported caffeine has the ability to reduce DOMS. They mesured perceived soreness in males consuming caffeine one hour before a workout. They found a lower level of soreness in the biceps on day 2 and 3 compared to a placebo after subjects completed a bicep curl protocol. Using a dosage of 5mg/kg bodyweight they found a beneficial effect of caffeine on soreness. For comparison, a 185lb (~84kg) male would take about 420mg of caffeine preworkout. That is a ton of caffeine! An 8oz Red Bull contains roughly 85mg. Does your preworkout supplement have that much caffeine? Probably not. If you’re wondering when caffeine peaks in the blood, it’s about one-hour post ingestion. Caffeine is an adenosine antagonist and affects the activity of central nervous system (CNS) by blocking adenosine receptors, thus resulting in decreased levels of soreness. This suggests that short-term caffeine ingestion before a strenuous workout may decrease overall soreness levels. However, the subjects who took caffeine were able to perform more reps than the control group, which could be a confounder.
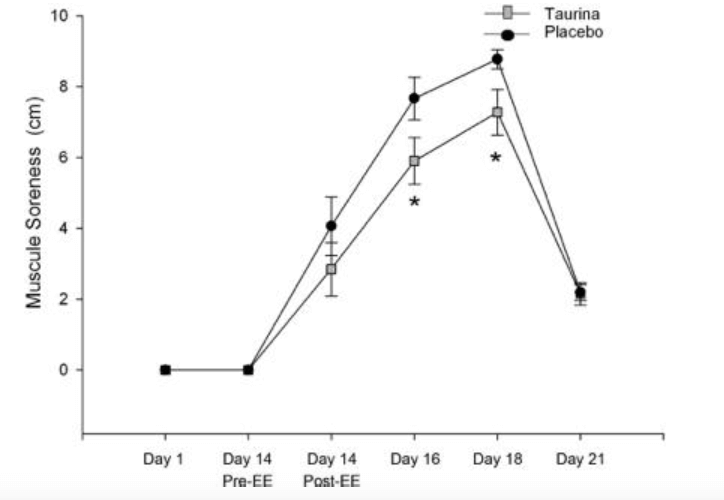 Taurine is found in muscle and has multiple biological functions. Remember that Red Bull I mentioned earlier? Well, it has about 1,000mg of taurine. For reference: Up to 3,000mg a day of supplemental taurine is considered safe. One double-blind study (10) of males completed over 21 days measured the effects of 50mg of taurine (20x less than the content in a Red Bull) after 7 days of eccentric exercise. The researchers found a reduction in DOMS and oxidative stress markers after exercise; however, there was no effect on inflammatory markers. Could this be a way to battle the other side? If inflammation is one component to DOMS and oxidative stress is another component, we need a study to combine the two. That probably won’t happen soon, but it would be fun to see if they were synergistic.
Taurine is found in muscle and has multiple biological functions. Remember that Red Bull I mentioned earlier? Well, it has about 1,000mg of taurine. For reference: Up to 3,000mg a day of supplemental taurine is considered safe. One double-blind study (10) of males completed over 21 days measured the effects of 50mg of taurine (20x less than the content in a Red Bull) after 7 days of eccentric exercise. The researchers found a reduction in DOMS and oxidative stress markers after exercise; however, there was no effect on inflammatory markers. Could this be a way to battle the other side? If inflammation is one component to DOMS and oxidative stress is another component, we need a study to combine the two. That probably won’t happen soon, but it would be fun to see if they were synergistic.
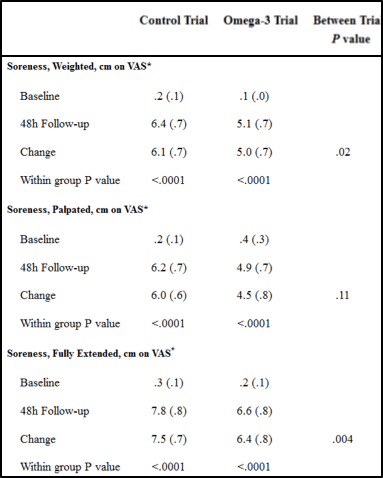
Omega-3 fatty acid is found in fish and is becoming increasingly used to fortify foods. You can also find EPA/DHA in those lovely pills that make you burp fish all day. Several studies reported positive effect of omega-3 fatty acids on DOMS, presumably due to the decrease in pro-inflammatory factors such as IL-6 and TNF-alpha. There are a ton of studies to show taking an omega-3 supplement is good for you in many ways, and this seems to hold true for DOMS. If you’re interested in the results, the main table from Jouris et al 2013 is below.
Cryotherapy, on the other hand, probably doesn’t reduce DOMS. This goes directly against the current trend of athletes jumping in a tube surrounded by liquid nitrogen to help recovery. Whole body cryotherapy exposes athletes to cold, dry air below -100C for between two and four minutes in a specialized chamber. A recent Cochrane Review by Costello et al., found that there was insufficient evidence to determine whether cryotherapy can reduce muscle DOMS or improve recovery.
No guidelines currently exist for its clinical effectiveness or for safe usage. Cryotherapy is thought to work by reducing temperature in the skin, muscle, and core. The theory is muscle soreness is relieved by reducing muscle metabolism, skin microcirculation, nerve conductivity and receptor sensitivity. In addition, it could have a placebo effect by reducing the subjective feeling of DOMS post-exercise. Using a meta-analysis based on four eligible studies, it seems cryotherapy does not reduce DOMS or improve recovery. Furthermore, insufficient evidence exists on whether this therapy could actually be harmful. We do know, however, that cold water emersion post-exercise can decrease rate of muscle growth. For the time being, cryotherapy and cold water emersion are probably two things you should avoid – you probably won’t recover any faster, and you may not build as much muscle.
Conclusion
Soreness can provide some insight, but don’t use it as a marker for a good workout. High levels of soreness indicate the lifter has exceeded the capacity for the muscle to undergo repair. Indeed, soreness can impede the ability to train properly, and it may decrease motivation.
The consensus among researchers is that there is no single component that causes DOMS. Instead, there are a number of complex events that may explain this phenomenon. It is the main cause of reduced exercise performance including decreased muscle strength and range of motion for both athletes and non-athletes. Common supplements to combat DOMS include caffeine, omega-3 fatty acids, and taurine.
Sources
- Sikorski EM, Wilson JM, Lowery RP, Joy JM, Laurent CM, Wilson SM-C, Hesson D, Naimo MA, Averbuch B, and Gilchrist P. Changes in perceived recovery status scale following high volume, muscle damaging resistance exercise. J Strength Cond Res 27: 2079–2085, 2013.
- Close, Graeme L., Tony Ashton, Tim Cable, Dominic Doran, and Don P. M. MacLaren. “Eccentric Exercise, Isokinetic Muscle Torque and Delayed Onset Muscle Soreness: The Role of Reactive Oxygen Species.” European Journal of Applied Physiology 91, no. 5–6 (May 2004): 615–21. doi:10.1007/s00421-003-1012-2.
- Stauber WT, Clarkson PM, Fritz VK, and Evans WJ. Extracellular matrix disruption and pain after eccentric muscle action. J Appl Physiol 69: 868–874, 1990.
- Flores, Débora F., Paulo Gentil, Lee E. Brown, Ronei S. Pinto, Rodrigo L. Carregaro, and Martim Bottaro. “Dissociated Time Course of Recovery between Genders after Resistance Exercise.” Journal of Strength and Conditioning Research / National Strength & Conditioning Association 25, no. 11 (November 2011): 3039–44. doi:10.1519/JSC.0b013e318212dea4.
- Trost Z, France CR, Sullivan MJ, and Thomas JS. Pain-related fear predicts reduced spinal motion following experimental back injury. Pain 153: 1015–1021, 2012.
- Paulsen, G, Mikkelsen, UR, Raastad, T, and Peake, JM. Leucocytes, cytokines and satellite cells: what role do they play in muscle damage and regeneration following eccentric exercise? Exerc. Immunol. Rev. 18: 42-97, 2012.
- Cheung, Karoline, Patria Hume, and Linda Maxwell. “Delayed Onset Muscle Soreness : Treatment Strategies and Performance Factors.” Sports Medicine (Auckland, N.Z.) 33, no. 2 (2003): 145–64.
- Proske U and Morgan DL. Muscle damage from eccentric exercise: Mechanism, mechanical signs, adaptation and clinical applications. J Physiol 537: 333–345, 2001.
- Zainuddin, Zainal, Mike Newton, Paul Sacco, and Kazunori Nosaka. “Effects of Massage on Delayed-Onset Muscle Soreness, Swelling, and Recovery of Muscle Function.” Journal of Athletic Training 40, no. 3 (September 2005): 174–80.
- Crane, Justin D., Daniel I. Ogborn, Colleen Cupido, Simon Melov, Alan Hubbard, Jacqueline M. Bourgeois, and Mark A. Tarnopolsky. “Massage Therapy Attenuates Inflammatory Signaling After Exercise-Induced Muscle Damage.” Science Translational Medicine 4, no. 119 (February 1, 2012): 119ra13-119ra13. doi:10.1126/scitranslmed.3002882.
- Sikorski, Eric M., Jacob M. Wilson, Ryan P. Lowery, Jordan M. Joy, C. Matthew Laurent, Stephanie M-C Wilson, Domini Hesson, Marshall A. Naimo, Brian Averbuch, and Phil Gilchrist. “Changes in Perceived Recovery Status Scale Following High-Volume Muscle Damaging Resistance Exercise:” Journal of Strength and Conditioning Research 27, no. 8 (August 2013): 2079–85. doi:10.1519/JSC.0b013e31827e8e78.


