
Prefer to listen? Check out the podcast episode on this topic.
Want to hear Eric and Greg discuss the key takeaways from the caffeine literature? Check out the podcast episode they recorded about caffeine and health and sex-based caffeine differences. The episode also contains an interview with IPF World Champion Natalie Hanson. Listen below, or subscribe on Apple Podcasts, Google Podcasts, Stitcher, or wherever you get your podcasts.
Caffeine (1,3,7-trimethylxanthine) belongs to a group of compounds called methylxanthines, which are primarily known for their stimulatory effects. In nature, caffeine serves as a natural pesticide that plants produce to keep insects from eating them. In the modern human diet, caffeine is a remarkably common component of numerous foods and beverages, and recent estimates suggest that up to 85% of US adults regularly consume caffeine. Average adult caffeine intakes vary among countries; Americans consume about 186mg per day, while the estimate is 260mg per day in Japan, and is likely higher in the world’s leaders in coffee consumption, including Finland, Norway, the Netherlands, and Sweden.
Caffeine finds its way into tea, coffee, soft drinks, chocolate, and medications, in addition to most pre-workout supplements on the market. Aside from being present in some delicious foods and beverages, caffeine has long been touted as a performance-enhancing supplement. If true, that would be pretty cool, because there aren’t many ergogenic ingredients with potential to sneak their way into your diet via affordable, easily accessible sources that taste great. However, it’s only cool if caffeine actually does enhance performance in a safe and reliable manner. This article discusses what caffeine does in the body, how it affects strength performance, and whether or not health and safety concerns about caffeine are warranted.
How might caffeine improve strength?
Before discussing the studies evaluating the strength effects of caffeine, it’s important to know how caffeine is supposed to work. It’s hard to critically evaluate a body of literature if you don’t really know what you’re looking for or why you should expect to find it. Humans have been consuming caffeine for ages, and we’ve been studying it for an impressively long time. As reviewed by Perkins and Williams, there are formal research reports about caffeine’s ergogenic properties dating all the way back to 1893. As early as 1939, scientists were calling for bans of highly concentrated caffeine products in athletic competition. Despite this rich history of caffeine research, there’s still a bit of confusion pertaining to the mechanisms by which it may enhance performance.
Catecholamines
In terms of modern caffeine research, much of the early work investigated aerobic endurance exercise outcomes and the mechanisms underlying such performance effects. Interest was focused almost exclusively toward peripheral mechanisms occurring outside of the central nervous system (CNS). For example, there were studies showing that caffeine increased the catecholamine response to exercise, resulting in higher blood concentrations of epinephrine (adrenaline) and norepinephrine (noradrenaline). While dopamine is also a catecholamine, the exercise literature tends to focus on epinephrine and norepinephrine because their exercise-induced changes are large and easy to measure, and they are known to have widespread effects throughout the body that are relevant to exercise, such as bronchodilation, tissue-specific vasodilation and vasoconstriction, carbohydrate and fat mobilization, and increased cardiac output.
In the caffeine research, one of the prevailing theories was that catecholamines increased glycolytic flux by enhancing glucose availability and stimulating glycolysis, thereby enabling the body to sustain high power output by utilizing carbohydrate more effectively for energy. This premise is indirectly supported by a number of studies showing increased blood glucose following caffeine ingestion, and studies showing simultaneous increases in lactate production and performance. Unfortunately, as reviewed by Davis and Green, it doesn’t seem like this hypothesis adequately explains the performance effects of caffeine. While there is little doubt that catecholamines can contribute to some of the numerous physiological effects we observe following caffeine ingestion, such as enhanced alertness, increased heart rate, and elevated blood pressure, they’re unlikely to be the primary driver of performance improvements. There are studies showing caffeine to increase catecholamine levels and improve performance in the absence of increased glycolytic flux, studies showing increased glycolytic flux in the absence of increased catecholamines, increased catecholamine levels have not consistently been shown to yield performance improvements, and performance improvements with caffeine have been observed in the absence of substantial catecholamine changes. In short, the theory sounds great, but the evidence doesn’t support it in a reliable manner.
Fat oxidation and glycogen sparing
In the early caffeine literature, it became apparent that caffeine was particularly helpful for increasing performance of prolonged endurance activities. It was speculated that caffeine might have been enhancing fat oxidation, thereby saving glycogen for when it was truly needed during prolonged exercise. Caffeine certainly causes an acute increase in free fatty acid mobilization; this is likely caused by a combination of antagonism of A1-adenosine receptors and catecholamine release. While caffeine has been shown to inhibit phosphodiesterase in vitro, and phosphodiesterase inhibition would enhance lipolysis and sparing of glycogen, it’s unlikely that a person would consume caffeine at a high enough dose to meaningfully inhibit phosphodiesterase. Nonetheless, the idea that enhanced fat oxidation (and subsequent conservation of glycogen) dictates the performance benefits of caffeine is pretty incomplete. While some studies have shown caffeine to reduce glycogen utilization during exercise, this finding is somewhat inconsistent. More importantly, this explanation fails to explain how caffeine has (on many occasions) enhanced performance of activities that are not limited by glycogen availability, and does very little to explain how caffeine would enhance performance of high-intensity, short-duration strength and power exercise in which fat oxidation is pretty much negligible during the bout.
Sodium/potassium pumps
Another potential peripheral mechanism pertains to the regulation of sodium and potassium balance within the muscle. Muscle fatigue is complex and multifaceted, but maintaining an appropriate balance of sodium and potassium within the muscle is critical to ensuring that muscle force can be maintained during repeated muscle contractions. Sodium/potassium pumps function to continuously restore balance, but not with perfect efficiency; as such, plasma potassium levels increase as exercise intensity increases. As potassium is increasingly relocated outside of the muscle, resting membrane potential of muscle cells is reduced, which can impair the ability to further complete forceful muscle contractions. Catecholamines and caffeine metabolites have both been shown to directly increase the activity of sodium/potassium pumps, which led researchers to believe that caffeine may improve performance by facilitating the restoration of normal sodium and potassium balance within the exercising muscle. If increased activity of sodium/potassium pumps was a primary mechanism driving caffeine-induced performance improvements, we could reasonably expect to observe that caffeine would lower plasma potassium levels during exercise, this effect would be more pronounced during exercise of higher intensities, and the ergogenic effect of caffeine would similarly be more pronounced during high-intensity exercise.
While some studies have shown caffeine to reduce plasma potassium concentrations at rest or during exercise, this effect has been fairly inconsistent and appears to be either similar or lesser in magnitude during high-intensity exercise. Furthermore, the ergogenic effects of caffeine seem to be larger and more reliable during steady-state aerobic exercise in comparison to strength and sprint outcomes of higher relative intensity and shorter duration. Taken together, it seems unlikely that caffeine primarily enhances strength performance by increasing sodium/potassium pump activity.
Adenosine antagonism
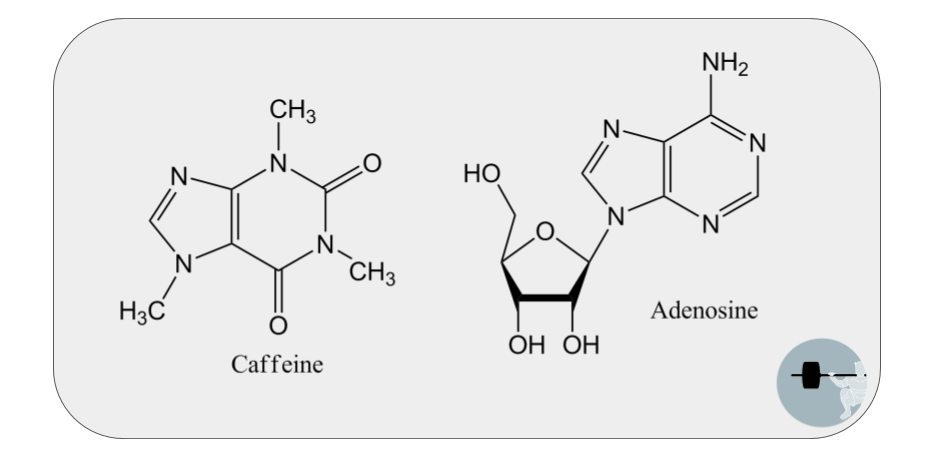
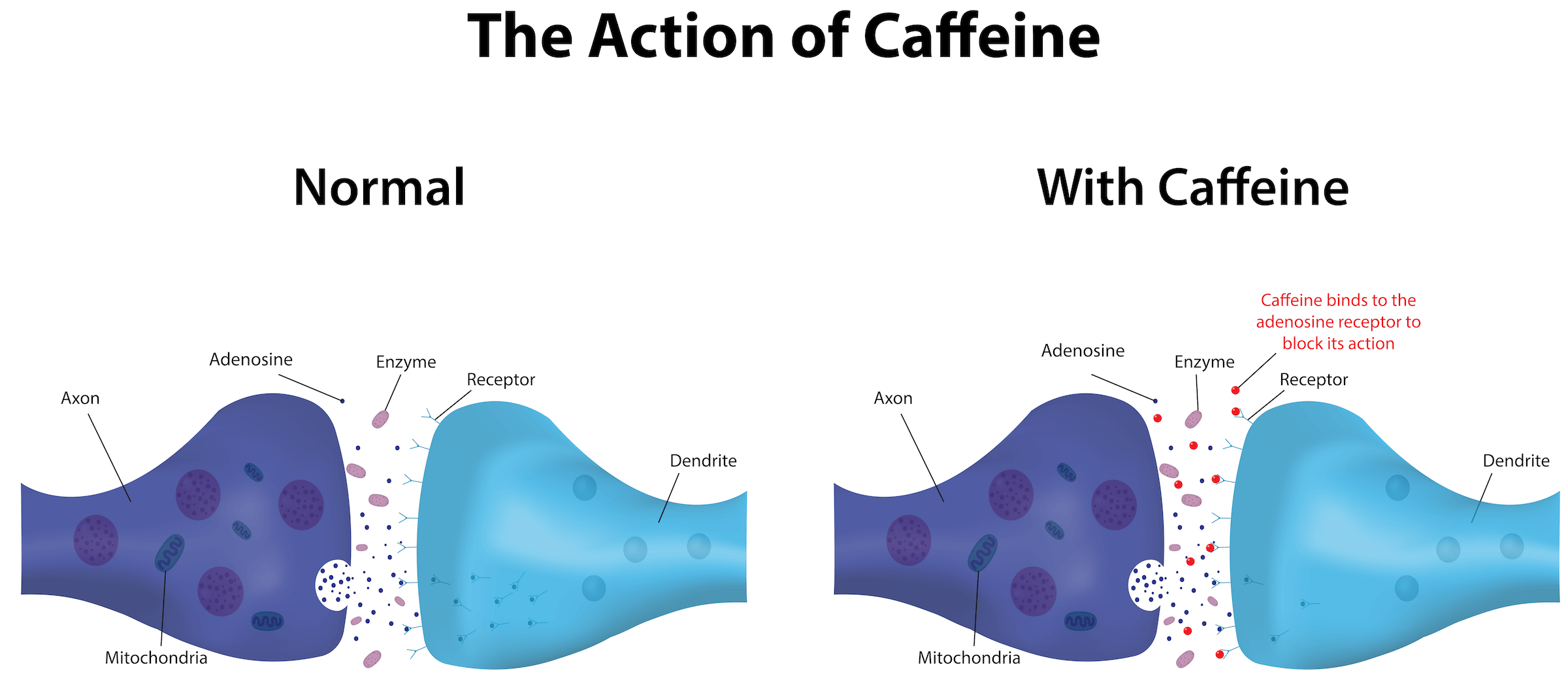
The scientific consensus is moving toward the conclusion that caffeine is mainly enhancing performance outcomes by influencing the CNS. Caffeine has a structure that is very similar to adenosine; so similar, in fact, that it can bind to adenosine’s receptors (Figure 1). This is called competitive antagonism or competitive inhibition, because adenosine’s ability to bind is impeded when caffeine temporarily “steals” its receptors. There are four subtypes of adenosine receptors that are present in various tissues throughout the body, but caffeine’s effects are mostly attributable to its binding to the A1 and A2A adenosine receptors in the brain. Antagonism of adenosine receptors is the primary driver of many of caffeine’s fairly obvious effects: increased heart rate, blood pressure, wakefulness, and alertness. When it comes to exercise, antagonism of adenosine receptors also results in less perceived pain, less perceived exertion, and enhanced maintenance of motor unit firing rates. The result is an improved ability to produce high forces and maintain power output during fatiguing exercise, thus enhancing fatigue resistance in a variety of tasks that include strength and sprint exercise.
Muscle calcium release
While adenosine antagonism certainly seems to be the primary driver of caffeine’s performance-enhancing effects, it doesn’t appear to explain everything. A great example of this is a pretty groundbreaking study completed by paraplegic and tetraplegic participants using electrically stimulated muscle contractions for exercise testing. With this model, the researchers were able to evaluate the peripheral response to caffeine ingestion, while minimizing the brain’s influence on motor control and the perception of pain and fatigue. Even under these circumstances, caffeine enhanced muscular endurance by 6%. The authors concluded that some peripheral mechanism must have elicited the observed improvement, speculating that the mechanism might involve calcium transport within the muscle. When muscles receive a signal to contract, the release of calcium from the sarcoplasmic reticulum is the critical step that precedes force production, and diminished calcium release results in diminished force production. As reviewed by McLellan et al, there is some evidence that caffeine can increase sarcoplasmic reticulum calcium release, thereby enhancing muscle force production and resistance to fatigue during multiple contractions.
In summary, there are very plausible mechanisms by which caffeine might enhance strength performance. While much of the early caffeine literature focused on catecholamines, fat oxidation, and glycogen sparing, the consensus is that adenosine antagonism is the primary driver of performance enhancement (Figure 2), with some secondary peripheral mechanism(s) that may relate to muscle calcium handling. This is great, because both of those should theoretically translate from aerobic exercise to strength exercise. But do they?
What types of exercise performance are improved by caffeine?
Endurance exercise
Costill and colleagues reported that coffee increased time to exhaustion during cycling (at 80% of VO2max) all the way back in 1978. In the decades since, several more trials have been conducted to evaluate the effects of caffeine on endurance exercise. In recent years, a number of meta-analyses have aggregated the results from these decades of research. If you’re unfamiliar with meta-analyses, they essentially gather up a large number of studies with similar methods and mathematically combine their results. While there are some shortcomings and imperfections, an effectively executed meta-analysis gives us a great summary of the available literature on a topic.
A recent meta-analysis aggregated the results of 44 studies that evaluated the effect of caffeine on time trial performance. Caffeine was found to reduce time to completion by about 2%, with a standardized effect size (Hedges’ G, to be specific) of about 0.28. In “real world” terms, reduced time to completion is like measuring how long it’d take to finish a race, so a reduction is a good thing. Mean power output during time trials was increased by about 3% with caffeine intake, which corresponded with an effect size of 0.22. Notably, the authors pointed out that there seems to be a great deal of variability in caffeine responses, with a handful of studies actually reporting slightly better performance in the placebo condition than the caffeine condition. As noted by Grgic et al, there are actually several meta-analyses out there when it comes to caffeine and endurance exercise. Generally speaking, caffeine enhances endurance performance on a variety of aerobic exercise tasks with reported effect sizes range from 0.2-0.6, which would typically be classified as a small to moderate effect.
Strength and power
“Strength and power” is a pretty broad category that encompasses a wide range of outcomes. In 2018, I helped out with a meta-analysis specifically looking at one-rep max (1RM) strength and vertical jump power. We found that caffeine significantly improved vertical jump power (ES = 0.17) and 1RM strength (ES = 0.20). This finding for jump power mirrors a separate meta-analysis looking at Wingate performance. If you’re not familiar with the Wingate test, it’s a brutal, 30-second cycling test that involves cycling as hard as possible against a fairly high resistance level. If you were to design a test solely for the purpose of making someone vomit from exertion, the Wingate would be that test. Caffeine was found to enhance both peak (ES = 0.27) and mean (ES = 0.18) power output during Wingate sprints, reinforcing the idea that caffeine enhances power-oriented outcomes. When it comes to the strength finding from our meta-analysis of 1RM strength, our results matched up quite well with a meta-analysis from 2010. Their study evaluated the effects of caffeine on maximum voluntary contraction strength, which included the peak force achieved during a single isometric or isokinetic maximal contraction, in addition to 1RM outcomes. They also found caffeine to have a positive effect, with an effect size of 0.19. In comparison to maximal strength, caffeine’s effects on muscular endurance (such as the number of repetitions completed prior to failure) seem to be larger, with a 2016 meta-analysis reporting an effect size of 0.38.
If you’re interested in taking a very “big picture” look at the caffeine literature, an umbrella review was recently published in the British Journal of Sports Medicine. This is basically a review of the meta-analyses in the literature, or a “review of reviews.” As a whole, the caffeine research to date seems to show, fairly conclusively, that caffeine has a larger effect on aerobic endurance exercise in comparison to strength and power outcomes. The effects on muscular endurance are smaller than the effects on aerobic endurance, and the effects on maximal strength and anaerobic power output are even smaller. Nonetheless, caffeine does appear to enhance maximal strength and peak power to a small but statistically significant extent. What we still don’t know, however, is whether or not these acute (single-session) performance improvements from caffeine translate to meaningful strength and hypertrophy gains over time. As far as I know, the only studies looking at long-term training adaptations over several weeks of pre-training caffeine supplementation are studies involving multi-ingredient pre-workout supplements, which are confounded by the presence of several other ingredients that make it impossible to determine caffeine’s independent contribution. Until longer studies are conducted using caffeine in isolation, we simply don’t know. And, as discussed in a later section, the possibility that caffeine’s performance-enhancing effects wear off with repeated use may limit its utility as an everyday training aid.
Effect sizes aren’t necessarily the most intuitive values to interpret on their own, but they allow us to compare different supplements on somewhat equal footing. When it comes to strength and power outcomes, creatine is still in a class of its own. It seems that there is a second “tier” of supplements forming; a group of supplements that exert tangible, meaningful effects that aren’t quite as large as those of creatine. Obviously it depends on the exact exercise task you’re hoping to improve, but this second tier is where we see supplements like beta-alanine, sodium bicarbonate, and possibly (pending further evidence) citrulline malate and dietary nitrate. For high-intensity exercise outcomes, caffeine fits comfortably within this second tier of supplements.
How to use caffeine: dose, source, and timing
Dose
The dosing recommendations for caffeine are pretty straightforward. Doses less than 3 mg/kg of body mass (such as a morning cup of coffee) can certainly enhance wakefulness and alertness, but they often aren’t enough to get the job done when it comes to enhancing exercise performance. Research showing performance benefits tends to provide doses ranging from 3-6 mg/kg, and most studies tend to stay on the higher end of this range (5-6 mg/kg), just to be safe.
It’s important to highlight that this ends up being a pretty large dose. If you weigh 100kg (220lb), this means that you’d be given a 600mg caffeine dose in most studies, which is about 6 cups of brewed coffee, all at once.
Studies investigating up to 13 (!) mg/kg of caffeine have reported that the performance benefits seem to peak around 5-6 mg/kg, with no substantial additional benefit observed at higher doses. More importantly, a lot of people get really uncomfortable at doses above the 5-6 mg/kg range. For example, one study found that endurance exercise performance was enhanced by doses of 3 and 6 mg/kg, but not with 9 mg/kg. In a different study investigating doses of 3, 6, and 9 mg/kg, the researchers found that 7 out of 10 women ingesting a dose of 9 mg/kg reported adverse effects such as tremors, dizziness, vomiting, and profuse sweating. Taken together, it would appear that doses beyond 6 mg/kg yield no additional performance benefit and might even have a detrimental effect on performance by inducing uncomfortable side effects.
Source
Coffee is cheap, delicious, and accessible all over the place. For these reasons, it’d be fantastic if we could get ergogenic doses of caffeine from an ordinary cup of coffee.
Back in 1998, Graham et al set out to determine if coffee was able to get the job done. Nine subjects completed the study, in which endurance exercise (running to exhaustion at 85% of VO2max) was tested after ingestion of various test treatments. The treatments included:
- Placebo capsule + water
- Caffeine capsule + water
- Regular coffee
- Decaffeinated coffee
- Decaffeinated coffee + caffeine capsule
All treatments included 7.15 ml/kg of fluid, and caffeinated treatments all provided 4.45 mg/kg of caffeine.
Results of the study were quite surprising. Participants had significant performance improvements when they consumed water + caffeine capsules, but not when they consumed any other treatment. This means that caffeine’s benefits were somehow blunted when consumed as normal coffee, and even when the very same caffeine capsules were consumed with decaffeinated coffee. The authors hypothesized that some component of coffee, such as chlorogenic acid, interfered with the performance-enhancing benefit of caffeine.
This outcome was largely taken at face value for about 10-15 years after its publication, and notable review papers concluded that caffeine anhydrous, consumed in powder or capsule form, was more ergogenic than coffee. However, this result is a bit difficult to swallow. For example, why would Costill’s classic 1978 paper document performance-enhancing benefits of caffeine, given that their caffeine source was actually coffee?
Replication is a key, foundational principle of science, especially in fields in which small samples are common. Consider the following scenario: I flip a coin 10 times, and each flip can yield “heads” or “tails.” Theoretically, I should get 5 of each. But if I got 3 heads and 7 tails, that would be far from impossible, and not even particularly improbable. Obviously, no one would walk away from that experiment concluding that you have a 30% chance of getting “heads” when you flip a fair two-sided coin. We need to replicate that finding by doing another set of 10, and another, and another. If you get to 10,000 flips and find that you only got 3,000 heads, it’s a virtual certainty that there’s something strange going on with that coin. Small-sample research should be viewed with the same level of skepticism until a decent number of studies have been conducted.
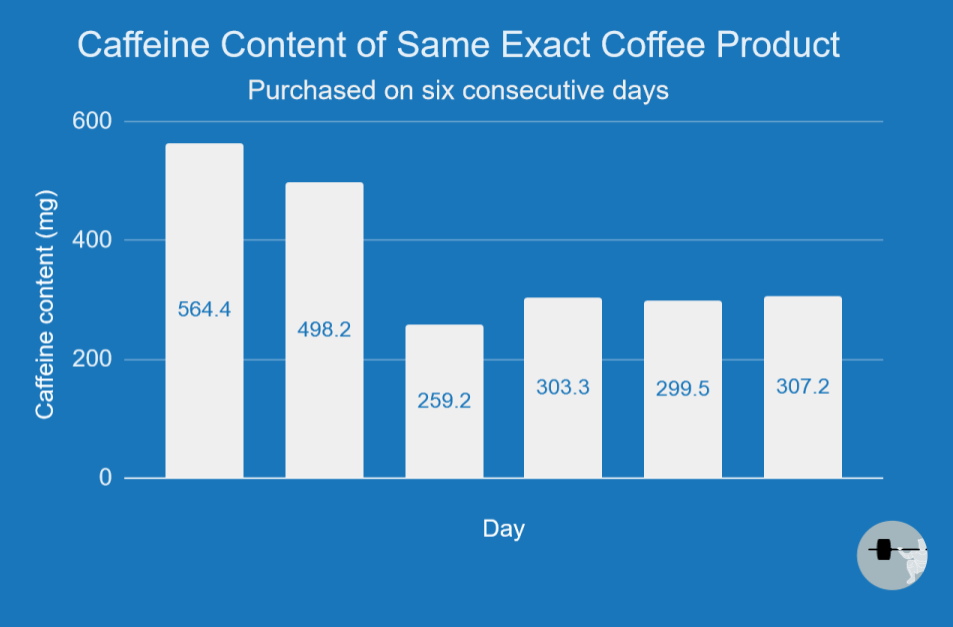
Hodgson et al directly compared caffeine anhydrous to coffee in the context of endurance performance in 2013, and my lab did a similar comparison in the context of strength and sprint performance in 2016. In both cases, caffeine anhydrous and coffee appeared to affect exercise outcomes in a similar manner. Also in 2016, Richardson et al showed that both coffee and decaffeinated coffee + caffeine anhydrous are capable of enhancing resistance exercise performance. Taken together, the current literature suggests that coffee exerts similar effects on performance as caffeine anhydrous, and coffee can therefore be considered a perfectly suitable source of caffeine for performance enhancement. There is, however, a big challenge when making coffee your caffeine source of choice: the caffeine content of brewed coffee is highly variable. Obviously caffeine content will vary based on the exact coffee bean, roast type, and preparation method, but seemingly thorough attempts to account for these factors can still result in an uncertain caffeine dose. Researchers conducting one study (Figure 3) purchased the same brewed coffee product at the same store for six days in a row, and found that the caffeine content ranged from 259mg to 564mg per dose!
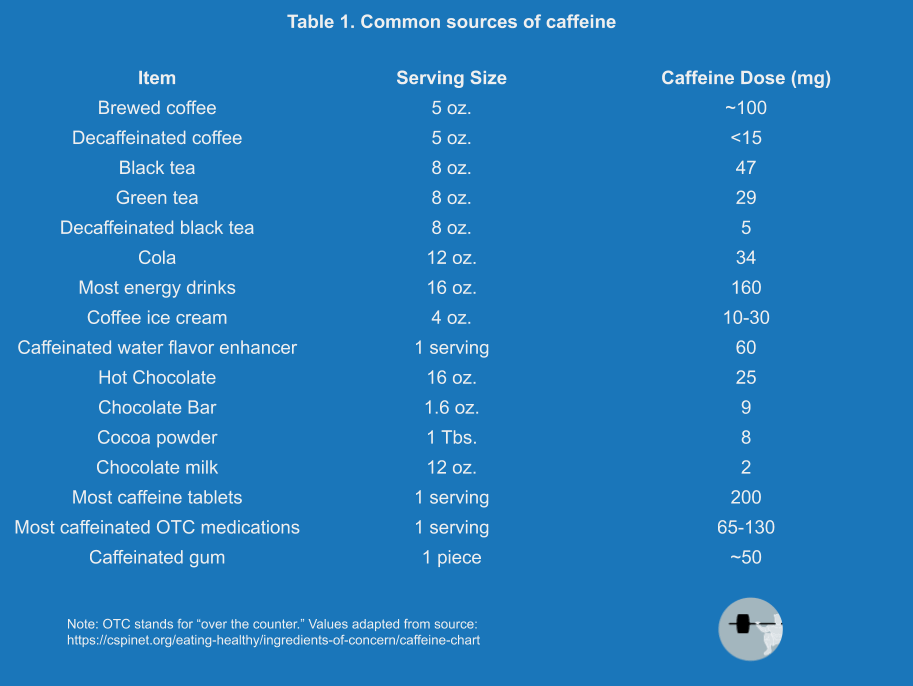
It’s worth noting that caffeine capsules and coffee are far from the only potential sources of caffeine (for a list of some common caffeine sources, see Table 1). As reviewed in a textbook chapter I helped write a few years ago, there have been a few studies looking at various absorption rates with different types of caffeine sources. Generally speaking, there’s not a meaningful difference when it comes to how rapidly blood caffeine levels are increased in response to coffee, tea, soft drinks, energy drinks, caffeine capsules, or caffeine powder when equivalent caffeine doses are orally ingested. Any differences in absorption rates between these sources are small in magnitude and likely related to differences in the pH, volume, and concentration of fluid consumed. The one exception would be caffeinated gum; caffeine can be absorbed (to some extent) through the oral mucosa, so caffeinated gum increases blood caffeine levels more rapidly than regular oral ingestion of a caffeinated product. That’s not particularly important, it just means you wouldn’t have to wait as long for caffeinated gum’s effects to kick in. Speaking of which, how long should you be waiting?
Timing
Caffeine has pretty high bioavailability; around 99% of orally ingested caffeine is absorbed within 45 minutes of ingestion, and less than 2% of orally ingested caffeine is excreted in the urine in an unchanged form. In the process of caffeine metabolism, it is broken down into three primary metabolites: paraxanthine (80%), theobromine (11%), and theophylline (5%), with the remainder of caffeine being broken down into a number of less plentiful metabolites. The majority (about 95%) of caffeine metabolism is dictated by the CYP1A2 enzyme, which is part of the liver’s cytochrome P450 enzyme system. After oral caffeine ingestion, substantial increases in blood caffeine concentrations are observed within 15 minutes, and peak values are typically reached within about 30-60 minutes. However, it could take up to 2 hours in some cases, as the rate of gastric emptying and the presence of other nutrients can certainly affect the rate of caffeine appearance in the blood. If caffeine is ingested as gum, the absorption rate is about 30-50% faster, give or take. The half-life of caffeine (the time required to clear half of the dose from your bloodstream) is generally estimated to be around 3-6 hours, but singular studies have suggested that the number may be as low as 2 hours or as high as 12 hours.
Clearly, there is a great deal of variability when it comes to the rate at which caffeine is metabolized. The CYP1A2 enzyme is largely responsible for caffeine metabolism, and up to 72.5% of the variability in CYP1A2 enzyme activity is determined genetically. We all get our alleles for the CYP1A2 gene from our biological parents, and we’ve got three options: we could get two copies of the “A” allele, two copies of the “C” allele, or one of each. People with the “AA” arrangement are considered fast metabolizers, while individuals with “AC” or “CC” genotypes are considered slow metabolizers.
While CYP1A2 genotype certainly helps explain some of the variability in observed half-lives, it might also explain some of the variability in performance. While the science is far from settled, a recent study found that caffeine had an ergogenic effect in “AA” participants, no benefit for “AC” participants, and caffeine actually made endurance performance worse in the “CC” participants. It has been hypothesized that caffeine’s metabolites might make a meaningful contribution to the ergogenic effect of caffeine; as such, differing rates of caffeine metabolism could alter the rate at which metabolites accumulate, thereby altering the likelihood of observing an ergogenic effect. Such a hypothesis could possibly mean that slow metabolizers may simply need different dosing or timing recommendations to obtain performance benefits, but there is insufficient evidence to make a definitive conclusion at this time.
To make matters more complicated, there is a high likelihood that caffeine responses are mediated, to some extent, by variations in other genes. Some likely candidates include the ADORA2A gene, which codes for the adenosine A2A receptor, and a variety of genes that code for proteins involved with multiple neurotransmitter systems in the brain. Rate of caffeine metabolism is also influenced by several factors other than genotype. To varying degrees, CYP1A2 enzyme activity can be influenced by sex, estrogen level, menstrual cycle phase, oral contraceptive use, body composition, alcohol, flavonoids, grapefruit juice, numerous vegetables, charred meat, smoking, and a wide variety of prescription and over-the-counter drugs.
Taken together, the evidence would collectively suggest that caffeine should be consumed 30-90 minutes before exercise if you’re hoping to receive an ergogenic benefit. Generally speaking, 45-60 minutes before exercise offers a more specific recommendation that is usually fine for most circumstances. However, as discussed in this section, there can be a great deal of variability in the rate at which caffeine is metabolized, which has implications for the timing of caffeine dosing.
Synergistic ingredients
While on the topic of how to use caffeine, there are a few notable ingredients that appear to pair very well with caffeine. While we already know that epinephrine and norepinephrine tend to increase in response to caffeine ingestion, resulting in increased arousal and alertness, dopamine is another catecholamine that is often overlooked in the exercise science literature. Dopamine appears to play an important role in many of caffeine’s cognitive effects. There are antagonistic interactions between adenosine and dopamine; by antagonizing adenosine receptors, caffeine may therefore enhance dopamine release and/or dopaminergic neurotransmission. This is important because L-tyrosine is a building block from which dopamine, epinephrine, and norepinephrine are formed. Tyrosine is known to have some cognitive effects of its own, with some studies showing positive effects on memory, cognitive performance, perceived stress, and subjective well-being when exposed to acute stressors.
While L-tyrosine will not necessarily increase resting catecholamine production, it appears to exert its favorable cognitive effects by attenuating acute, stress-induced depletion of catecholamines. There isn’t much research directly assessing the combination of caffeine and L-tyrosine; while combination with L-tyrosine is unlikely to do much for exercise performance, it’s probably not a terrible idea to ensure that you have a nice reserve of the building blocks for catecholamine production present, especially if you’re primarily using caffeine to enhance alertness and cognitive function. Much of the L-tyrosine research uses fairly high doses, often around 150 mg/kg of body weight, when evaluating the effects of L-tyrosine alone. While there isn’t much research to make conclusions about adequate dosing when used as a supplement to support caffeine’s effects, I would speculate that much lower doses are sufficient, and I usually take around 1-2g when using caffeine.
L-theanine is a non-proteinogenic amino acid found primarily in green tea. When evaluating L-theanine on its own, some studies have documented positive effects on relaxation, anxiety, attention, and sleep quality. The cool thing about L-theanine is that its effects are remarkably complementary to some of caffeine’s “downsides.” Some people note that caffeine makes them a bit anxious, jittery, or too “amped up” to focus and perform well on cognitive tasks, and the potential for caffeine to disrupt sleep is well-documented. L-theanine can help attenuate some of these unfavorable responses to caffeine and can induce relaxation without sedation, meaning the L-theanine won’t counteract the intended effect of caffeine by making you tired. There are multiple human studies demonstrating that a combination of theanine and caffeine resulted in improvements in cognitive function and mood, and a rodent study found that theanine partially attenuated sleep disturbances caused by caffeine. Generally speaking, human studies combining theanine with caffeine tend to use theanine doses of around 100-200mg.
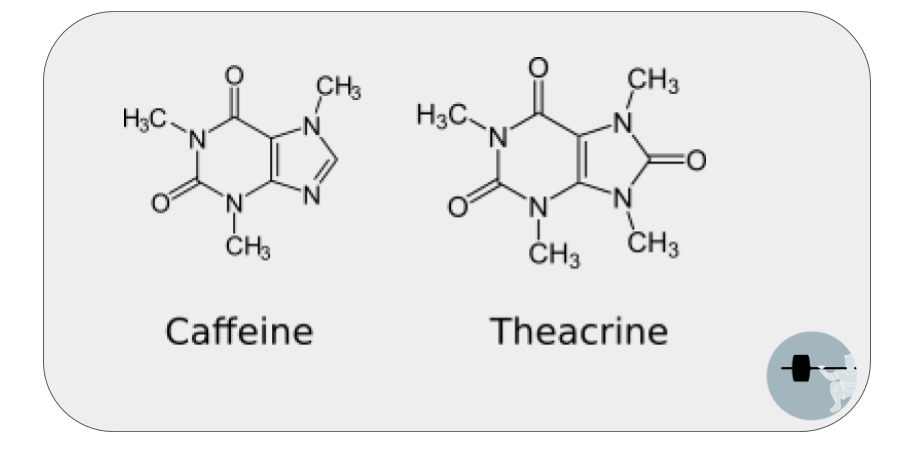
A third supplement that is sometimes combined with caffeine is theacrine, not to be confused with theanine, despite the similar spelling. Theacrine (1,3,7,9-tetramethyluric acid) is a purine alkaloid found in a very specific type of tea, and its structure is quite similar to that of caffeine (Figure 4). As a result, it appears to antagonize adenosine receptors and work through similar mechanisms of action. Studies investigating theacrine alone have documented effects like those observed with caffeine, such as perceived energy, focus, and concentration. A recent study evaluated both physical and cognitive performance using theacrine, caffeine, or a combination of both compared to placebo. All three treatments showed a trend for enhanced endurance performance compared to placebo, and both caffeine and caffeine + theacrine improved some indices of cognitive performance.
A cool thing about theacrine is that one study found that its effects didn’t seem to fade after 8 weeks of daily use; as discussed in the next section of this article, the same can’t be said for caffeine. Theacrine takes a slightly longer time to reach peak blood values when compared to caffeine (approximately 2 hours), and caffeine appears to enhance the bioavailability of theacrine when they are consumed together, whereas theacrine does not meaningfully influence caffeine pharmacokinetics. Theacrine has a substantially longer half-life than caffeine, with estimates ranging from 16.5-26.1 hours in one study (depending on the dose). Personally, I wish caffeine had a shorter half-life, so I don’t necessarily view a longer half-life as an unequivocally positive thing. On the bright side, it could potentially extend the period of time in which cognitive and/or physical performance are enhanced. But, for a stimulant, you could argue that the ideal scenario would be that you use it, you become alert for a set period of time, and then the stimulant quickly clears your system so you can get some sleep.
One of the downsides of caffeine is that you run the risk of disrupting sleep quality if you use it late in the day, as the half-life is generally around 3-6 hours. While a study found that 8 weeks of daily theacrine supplementation was not associated with any major safety concerns, they noted that self-perceived vigor was reduced at the 4-week time point. Given the long half-life of theacrine, I’d be interested to see more research evaluating the effects of theacrine on sleep quality, even when theacrine is consumed fairly early in the day. In addition, the authors of the paper noted that theacrine may have sleep-promoting effects at lower doses, as opposed to the wakefulness-promoting effects observed with higher doses. To make matters more uncertain, a rodent study found that theacrine paradoxically improved parameters of sleep quality and attenuated caffeine’s insomnia-inducing effect. Hopefully some human studies assessing theacrine’s effects on sleep duration and quality will be forthcoming; until that happens, it’s hard to make a definitive conclusion.
For now, there is reasonably strong theory to support the idea of combining L-tyrosine with caffeine, but more research is needed to confirm that this theory checks out in the real world. When it comes to L-theanine, there is some good human evidence demonstrating that it complements caffeine quite nicely. If you’re interested in some further reading on the topic, Ian McCarthy has written some informative lay press articles about stacking theanine and tyrosine with caffeine. There is emerging research suggesting that theacrine exerts effects similar to caffeine, albeit with a longer time to peak blood values and a longer half-life. The research also suggests that theacrine does not interfere with the effects of caffeine when they are combined and might be slightly more effective than caffeine alone, but more evidence is needed to conclusively show that theacrine actually provides additive, synergistic effects.
Do the effects of caffeine wear off over time?
If you’re a regular caffeine user, it’s quite apparent that some degree of habituation occurs. With consistent, repeated use, our bodies develop a tolerance to some of caffeine’s effects. There are a few mechanisms that likely contribute to this tolerance. As previously discussed, many of caffeine’s effects are primarily caused by caffeine blocking adenosine receptors; some rodent research has suggested that chronic caffeine use increases the number of adenosine receptors, thereby attenuating the magnitude of caffeine’s effects. There are also epigenetic changes that occur with repeated caffeine consumption. An epigenetic change refers to a change in gene function, without a change in the genetic code; you can think of it like using dimmer switches to turn the activity of different genes up and down. The epigenetic changes accompanying habitual caffeine use are likely to alter caffeine metabolism and clearance by influencing the activity of CYP1A2 (and other cytochrome P450 system genes), and likely to alter the response to caffeine by influencing genes in the dopaminergic and adenosine pathways. It’s pretty clear that certain responses to caffeine, such as effects on heart rate, blood pressure, alertness, and physiological arousal, are prone to the development of tolerance. But, do we become tolerant of caffeine’s ergogenic effects as well?
This question has been the focus of multiple research papers in recent years. For an in-depth discussion of this topic, be sure to check out Greg’s article in Volume 3, Issue 4 of Monthly Applications in Strength Sport (MASS). A lot of previous studies have addressed this question in a fairly indirect manner by grouping participants by habitual caffeine use based on their self-reported habits, then determining if caffeine was less effective for people who habitually consume it. These approaches have yielded mixed results, with some studies providing apparent evidence of tolerance formation, and others showing no signs of tolerance. More recently, a couple of studies have taken a more direct approach to this question by actually giving caffeine doses consistently over the course of 3-4 weeks. While the studies didn’t measure outcomes that the typical bodybuilder, powerlifter, or weightlifter would be most interested in, the results are informative nonetheless.
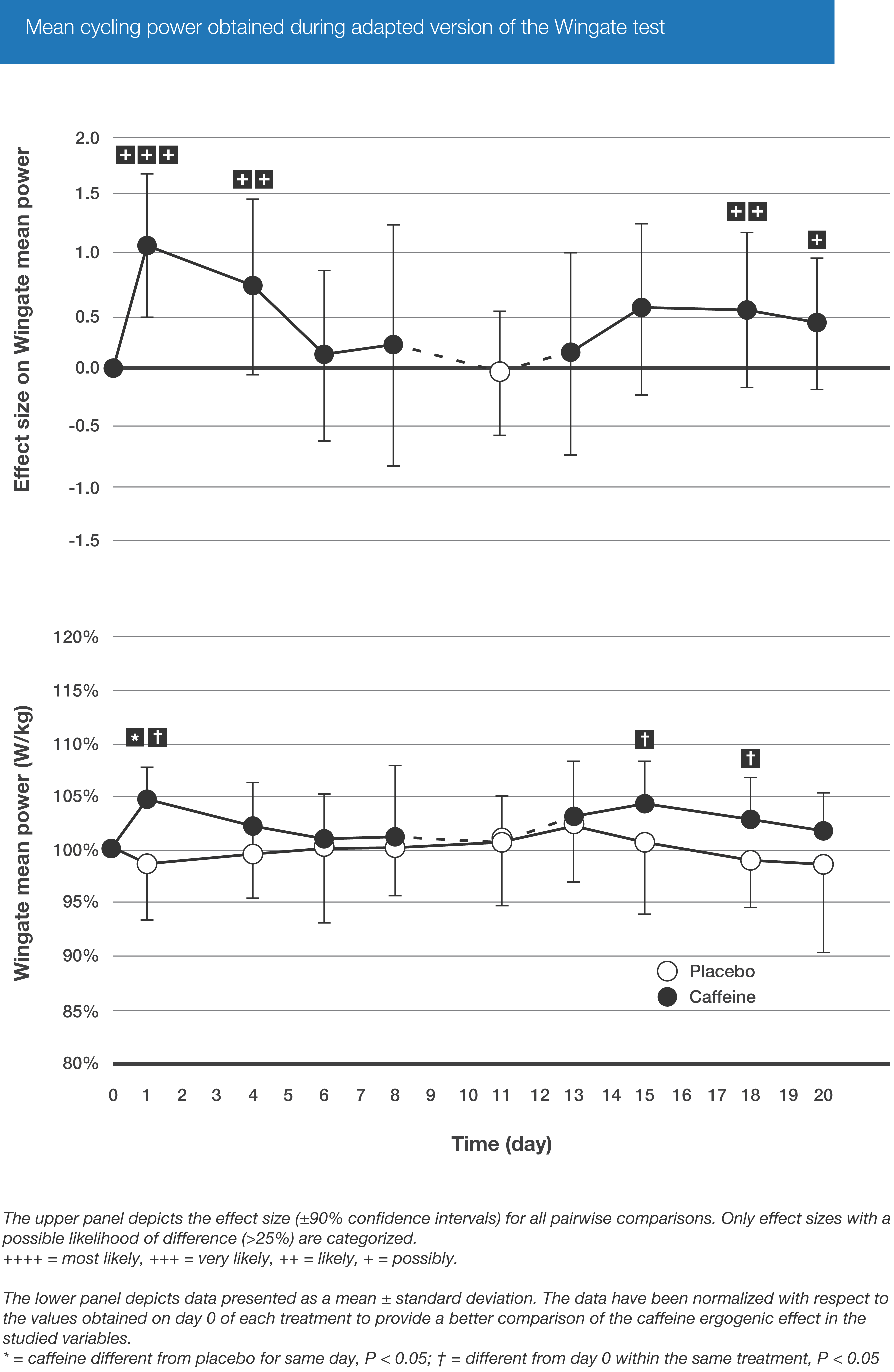
In one such study, caffeine’s effects on endurance cycling performance were diminished following 28 days of 1.5-3 mg/kg per day of caffeine ingestion, while a group consuming a daily placebo still enjoyed a performance-enhancing benefit from caffeine after the 4-week supplementation period. In another study, the effects of caffeine on both aerobic and anaerobic performance were consistently tracked over a 20-day period. Not all performance outcomes followed the exact same time course of habituation, but results generally suggested that caffeine’s ergogenic effects had faded a bit throughout the study (Figure 5). As discussed previously, this could potentially mean that the acute performance boost from caffeine may not persist when used as a daily training aid, which would reduce the likelihood that results from single-dose caffeine studies directly translate to enhanced training adaptations over time. As a result, caffeine may need to be used fairly strategically to translate acute performance boosts into long-term training adaptations. While this story is far from over, and more studies should be carried out to evaluate habituation effects using a variety of performance outcomes, supplementation durations, and caffeine doses, I agree with Greg’s conclusion: For now, it would be prudent to allocate your caffeine use thoughtfully if you’re interested in maximizing its ergogenic benefit. Such an approach would involve using caffeine only for your most important workouts or athletic events, or periodically taking some time away from caffeine (at least a couple of weeks, most likely) to resensitize your response before fully maximizing its performance-enhancing benefits.
When it comes to taking time away from caffeine, be sure to account for withdrawal. If you are a regular caffeine user and you abruptly stop using it, withdrawal symptoms will likely appear within 12-24 hours and reach peak intensity within about 20-48 hours. Symptoms typically include headache, drowsiness, fatigue, and irritability. It’s safe to assume that your athletic performance might take a slight hit during the peak of withdrawal symptoms, so it’d be wise to carefully decide the time at which you plan to cease caffeine use.
Common concerns
Cardiovascular health
The idea that caffeine is bad for the heart is a fairly pervasive misconception, which is probably fueled by two main drivers. First of all, a large dose of caffeine causes noticeable, acute changes in heart rate and blood pressure, especially for people who don’t regularly consume it. Intuitively, that might be perceived as an effect with eventual consequences. In addition, some early epidemiological studies reported links between coffee and cardiovascular disease, but many of these early studies failed to adequately account for the fact that coffee consumption is quite highly correlated with smoking.
Now, it’s worth noting that coffee and caffeine aren’t exactly the same thing. However, when you want to assess the long-term health effects of something, your best bet is to check the epidemiology literature. Unfortunately for us, there aren’t huge data sets looking at the effects of regular consumption of pre-workout supplements or caffeine capsules in tens of thousands of people over several decades. So, given the widespread use of coffee throughout the entire planet, the coffee literature is our best tool for assessing cardiovascular risk with long-term caffeine consumption. In studies that adequately control for smoking and other important factors, coffee consumption has not been associated with substantial increases in cardiovascular disease risk. In fact, studies generally tend to show that “moderate” coffee intake, often defined as somewhere between 1-5 cups per day, is actually associated with a reduction in risk. Beyond this intake, studies generally show that the health benefits disappear, but cardiovascular risk doesn’t seem to be meaningfully elevated when coffee intake is kept within fairly reasonable ranges.
As previously discussed, CYP1A2 genotype might influence the performance effects of caffeine by influencing the rate of caffeine metabolism. Similarly, authors have investigated the possibility that CYP1A2 genotype might influence caffeine’s effects on health-related outcomes. A 2006 paper found that coffee intake was associated with heart attack risk in slow metabolizers, but not in fast metabolizers. Similarly, a 2009 paper found that coffee intake was associated with hypertension risk in slow metabolizers, but not in fast metabolizers. While very preliminary research has suggested that the slow metabolizers are out of luck when it comes to cardiovascular outcomes and performance enhancement, there is one study suggesting that high caffeine intake is associated with lower bone density in elderly adults – but only in fast metabolizers. Nonetheless, it’s really important to note that all of these links between genotype and various health and performance outcomes are extremely preliminary in nature. For example, a recent (and very large) study found that moderate coffee consumption was associated with a protective effect for cardiovascular disease, whereas heavy (>6 cups per day) consumption was associated with a modest negative effect, and effects were not influenced by CYP1A2 genotype to a meaningful degree. To make matters a bit more complicated, the inconvenient truth of the matter is that caffeine metabolism is likely affected, to some extent, by several genes. As such, we are probably just scratching the surface when it comes to determining how our genes influence our body’s individualized response to caffeine intake.
For now, the most justifiable conclusion is that caffeine, consumed in coffee or tea, is unlikely to have devastating effects when it comes to cardiovascular health. It’s possible that some deleterious effects might be observed if you have particularly high caffeine intake (the equivalent of >6 cups of coffee per day, which is about 600 mg) or are a slow caffeine metabolizer, and we can’t rule out the possibility that effects are different if your primary caffeine source is something other than coffee or tea. Having said that, caffeine is not entirely benign in all contexts. Research suggests that high caffeine intake should probably be avoided by pregnant women, people with hypertension, elderly individuals at high risk for bone fracture, and anyone taking one of the many medications that are known to interact with caffeine. In addition, some people are particularly sensitive to caffeine and tend to be more susceptible to feeling jittery, anxious, or unable to sleep when moderate to large doses of caffeine are ingested. The acute lethal dose of caffeine is estimated to be around 10 grams (10,000 mg), but there’s no reason that anyone should ever be near that value, and it’d be unwise to approach it due to the well-known variability in caffeine metabolism between individuals. For example, there have been reports of fatalities from doses of 6.5 grams and lower, whereas a couple of college students were accidentally given 30 gram doses and (barely) survived, thanks to intensive care and dialysis. Generally speaking, research papers assessing the safety of caffeine tend to suggest that healthy adults ought to limit their daily caffeine to no more than roughly 400-600 mg/day, depending on body size.
Vasoconstriction/vasodilation
While we’re on the topic of the cardiovascular system, caffeine’s effects on blood vessels should be mentioned. Caffeine is an adenosine antagonist, and adenosine is known to have some vasodilatory effects, meaning it causes blood vessels to dilate and accommodate greater blood flow. From an exercise perspective, this sounds a bit problematic. Vigorous exercise requires that we deliver oxygen and energy substrates to the working muscle, and also demands that we have sufficient blood flow to clear out any localized accumulation of metabolites associated with fatigue. In fact, as discussed in a previous Stronger By Science article, many individuals supplement with nitric oxide precursors as a means of increasing blood flow during exercise. While one might intuitively assume that caffeine would therefore induce some blood vessel constriction that would be disadvantageous for exercise, the picture is (fortunately) a bit more complicated than that.
As highlighted in a 2010 review paper, caffeine affects the dilation and constriction of blood vessels in numerous, and sometimes conflicting, ways. Caffeine has both direct and indirect effects on a variety of physiological stimuli for both constriction and dilation of blood vessels, including adenosine, inositol triphosphate, and nitric oxide. The vascular effects of caffeine and adenosine both vary as a function of tissue type and duration of exposure. For example, adenosine induces vasodilation via A2A receptors in the coronary vasculature, but causes vasoconstriction via the A1 receptors in the pulmonary arteries and afferent arterioles of the kidneys. The overall vascular response to caffeine depends upon cellular events affecting the central nervous system, peripheral nervous system, kidneys, endothelial cells, and the smooth muscle cells that line blood vessel walls. Taken together, the authors of the review note that caffeine typically causes a mild and temporary constriction of blood vessels, but they primarily characterize caffeine as a vasodilator. This makes sense, given the fact that multi-ingredient pre-workout supplements containing caffeine have been shown to induce pretty substantial increases in blood flow. Obviously, such supplements contain other ingredients known to promote blood flow, but these findings suggest that any vasoconstriction induced by caffeine is not nearly robust enough to overpower contradictory signals that call for vasodilation. Blood flow is of paramount importance during exercise, so there are very powerful and redundant signals to ensure that blood flow is increased during exercise, with or without the addition of nitric oxide boosters. So, concerns about caffeine hindering a workout or ruining a “pump” by causing a meaningful degree of vasoconstriction seem to be pretty unfounded.
Dehydration
A common concern about caffeine is that it will actively contribute to dehydration. In reality, this concern is way overblown, for a couple of reasons.
It is certainly true that caffeine has a mild diuretic effect, meaning it increases urine output (and, therefore, fluid loss). However, the most common methods of ingesting large caffeine doses also involve fluid ingestion, such as drinking a cup of coffee or an energy drink. So, while a cup of coffee may slightly increase urine output, it also provides several ounces of water, and therefore has a net positive effect for hydration status. A 2016 study evaluated the hydrating effect of several beverages by monitoring fluid balance in the 4 hours following ingestion. The beverage hydration index of caffeinated coffee was lower than plain water, but not by much, and certainly not by a large enough magnitude to be concerned about. In addition, humans develop a tolerance to the diuretic effect of caffeine, to the extent that it becomes even more negligible in people who consume caffeine regularly.
Sleep
Given that caffeine clearly has a stimulant effect that promotes wakefulness, it’s quite intuitive to assume that caffeine consumption late at night could interfere with sleep. A study from 2013 evaluated the effects of caffeine intake (400mg) consumed 0, 3, or 6 hours before bed on various indices of sleep quality. Compared to a placebo, all three times of caffeine ingestion increased sleep disturbance and negatively impacted sleep quality. The important conclusion to draw from this study is not that you will avoid sleep disturbance by restricting caffeine within 6 hours of bed. This study tells us that consuming caffeine within 6 hours of bedtime is likely to disrupt your sleep, but it doesn’t tell us how long we actually have to abstain from caffeine to avoid sleep issues. It’s possible that you could avoid sleep disruption if the final dose is 7 hours before bed, 10 hours, 14 hours, or 24 hours. Frankly, it’s impossible to tell based on this study. The results suggest that the number is greater than 6 hours, but we can’t be certain how much greater. Realistically, the exact time of caffeine abstention needed prior to bedtime probably depends on the dose of caffeine, your habitual caffeine intake, how rapidly you metabolize caffeine, and how sensitive you are to the stimulatory effects of caffeine. As such, anyone with sleep issues should consider whether or not their caffeine intake habits might be contributing to their sleep disruption, even if they stop consuming caffeine fairly early in the afternoon.
Possible health benefits
While much attention has been devoted to potential adverse health effects of caffeine, it’s important to note that there are numerous health benefits associated with both caffeinated beverages (such as coffee and tea) and even caffeine itself. Both coffee and tea are loaded with antioxidants and other bioactive compounds, and decades of research suggests that regular moderate consumption of coffee and/or tea is associated with positive, protective health outcomes. Consumption of these beverages has been associated with reduced risk of mortality, certain cancers, liver conditions, depression, arthritis, type 2 diabetes, and other components of metabolic syndrome. As we’ve seen in some recent research, more antioxidants aren’t always better, and high-dose antioxidant supplementation has been shown to blunt adaptations to training. While the research has yet to identify an exact “dose” of antioxidant that would warrant concern regarding blunted training adaptations, the total amount of antioxidants provided by coffee and other whole food sources are substantially lower than the doses used in antioxidant supplementation studies, and the current consensus is that antioxidants obtained from non-supplementary diet sources are unlikely to counteract training adaptations.
There’s also some literature suggesting that regular consumption of caffeine is associated with lower risk of developing certain neurodegenerative diseases, including Parkinson’s and Alzheimer’s. The evidence for a reduction in Parkinson’s risk is a bit stronger than for Alzheimer’s, as the Alzheimer’s literature is fairly inconsistent. Interestingly, caffeine’s apparent reduction of Parkinson’s risk seems to be influenced by estrogen, with more pronounced effects observed in males and females who have never used post-menopausal hormone replacement. For now, there’s insufficient evidence to determine whether or not caffeine might play a role in slowing the progression of certain neurodegenerative diseases after diagnosis. In the case of Parkinson’s, there are numerous animal studies that detail some extremely plausible mechanisms by which habitual caffeine use could alleviate symptoms and slow down disease progression, but the limited number of human trials to date don’t paint a consistent picture from which to draw definitive conclusions. Oddly enough, one study found that caffeine did not significantly influence the rate of Parkinson’s disease progression, but the researchers observed faster progression of Parkinson’s disease among high caffeine consumers that also habitually used creatine. Given that this is just a single study and the authors are unable to identify a plausible mechanism underlying this observation, I file this finding under “interesting but unverified” for now.
In summary, caffeine was once widely perceived to have negative impacts on health, but this negative reputation has turned around significantly in the past couple of decades. It would appear that regular consumption of moderate caffeine doses, most commonly consumed as coffee or tea, has a neutral to positive effect on a wide range of health outcomes.
Summary
- Acute caffeine supplementation has a bigger effect on aerobic endurance performance than strength performance, but it still improves strength endurance and, to a lesser extent, maximal strength and power. There currently isn’t enough research to determine if these acute performance improvements translate to meaningful strength or hypertrophy gains over time.
- Most studies showing ergogenic effects use doses of 3-6 mg/kg of body mass, consumed about an hour before exercise.
- The performance benefits of caffeine seem to diminish (to some extent) over time, and it’s safe to assume that performance dips when a habitual caffeine user is experiencing caffeine withdrawal symptoms.
- There’s some justification that co-ingestion of L-tyrosine and L-theanine may support some of the more cognitively-oriented effects of caffeine ingestion, but more research is needed.
- The common health concerns pertaining to caffeine are fairly exaggerated within normal ranges of dosing (below 400-600 mg per day), and regular consumption of tea and coffee within this range are associated with neutral to positive effects on a wide range of health outcomes.
- Due to its fairly long half-life, it’d be a good idea to limit caffeine consumption late in the afternoon or evening.
- Genetic differences may impact the health and performance effects of caffeine. Key genes include CYP1A2 and ADORA2A, but many others are likely to play a limited role. This body of research is too small to draw definitive conclusions, but there is no doubt that caffeine’s performance benefits vary widely between individuals.
Supplement this article with the podcast episode on the topic.
Want to hear Eric and Greg discuss the key takeaways from the caffeine literature? Check out the podcast episode they recorded about caffeine and health and sex-based caffeine differences. The episode also contains an interview with IPF World Champion Natalie Hanson. Listen below, or subscribe on Apple Podcasts, Google Podcasts, Stitcher, or wherever you get your podcasts.
Read Next
- Not Another Boring Creatine Guide: Answers to FAQs and Lesser-Known Benefits
- Are Nitric Oxide Supplements Beneficial For Strength and Hypertrophy?


