
If you prefer to listen, we covered much of this article’s content in episode 132 of the Stronger By Science podcast, which you can listen to below. Alternatively, you can also listen on Spotify, Apple Podcasts or YouTube.
Until only a couple of years ago, full range of motion (ROM) was widely accepted as the best approach for trainees seeking to gain muscle. It wasn’t uncommon for ROM to be treated as an open-and-shut case. The only plausible reason to use a partial ROM was to use more weight and stroke your ego.
However, more recently, the concept of “long-length partials” or “lengthened partials” has been gaining steam.
In case you haven’t been following the hype, lengthened partials are simply partial ROM repetitions performed in the lengthened or stretched part of the movement. While there are many studies finding better muscle growth from lengthened partials than shortened partials – partial reps performed in the shortened/“peak squeeze” part of a movement (1, 2, 3, 4, 5, 6, 7, 8) – there are far fewer studies comparing lengthened partials to a full ROM (1, 2, 3, 4, 5). The most recent meta-analysis on the topic of ROM was performed by myself and some colleagues (1). At the time, there were only three studies comparing a full ROM to lengthened partials and measuring muscle growth (1, 2, 3). In a sub-group analysis, to see whether the muscle length mattered for muscle growth, we looked at only those three studies. Here are the results.
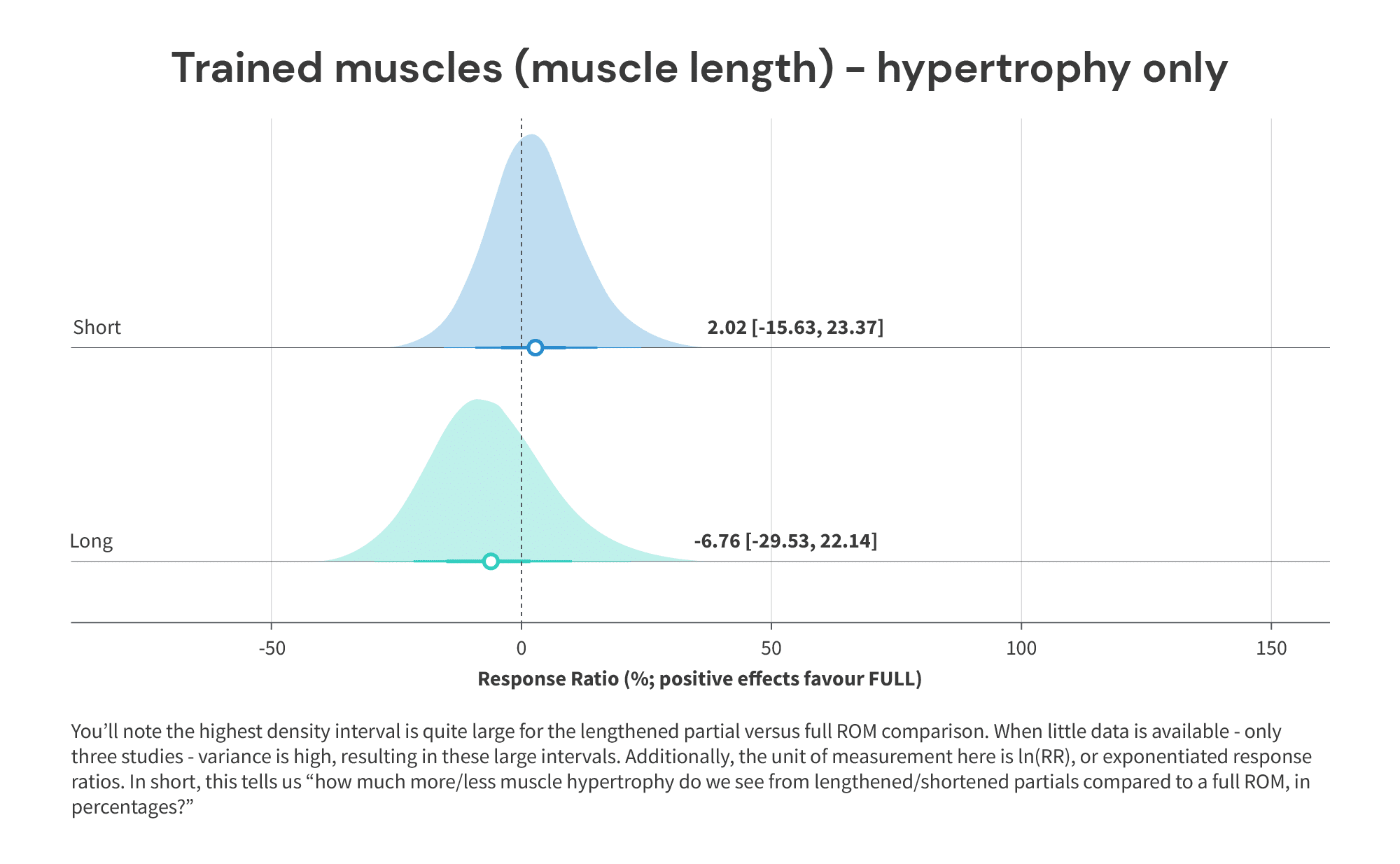
As you can see, lengthened partials were potentially better for muscle growth compared to a full ROM (6.76% more muscle growth, 95%CI -29.5 – 22.1). That said, a meaningful limitation of the data was the fact that there were only three studies to draw on. Fortunately, there has since been further research into the topic. First, a study by Kassiano et al (1) compared using a full ROM to lengthened partials (bottom half of the rep) to shortened partials (top half of the rep) in the leg press calf raise. The authors measured both lateral and medial gastrocnemius hypertrophy. Generally, the best hypertrophy outcomes were seen in the lengthened partial group, followed by the full ROM group, with the shortened partials group clocking in last, as you’d expect based on the results of the sub-group analysis above. Interestingly, the lengthened partials group saw approximately twice as much hypertrophy as the full ROM group at both the lateral and medial site (lateral gastroc: +7.3% versus +14.9%, medial gastroc: +6.7% versus +15.2%).
The second study to compare lengthened partials to full ROM was a study by Maeo and colleagues (1). Unfortunately, this study has only been presented at a conference. I reached out to the authors to see whether they had a full manuscript in the pipeline, but they haven’t gotten a chance to write up the results past the abstract-version yet. Fortunately, the authors are responsible for a good deal of the research in this area (1, 2), so I do still consider this study worthy of consideration. Maeo et al compared using a full ROM (90-0 degrees of hip flexion) to a lengthened partial ROM (90-45 degrees of hip flexion) on the multi-hip machine exercise. For those who don’t know what that is, it’s a similar movement pattern to a kickback. Notably, though, Maeo et al. instructed participants to minimize knee bend, making the movement closer to a hip hinge or Romanian Deadlift-type motion. They measured volume of the hamstrings and gluteus maximus using magnetic resonance imaging (MRI). In short, lengthened partials led to around twice as much hypertrophy of the hip extensors as full ROM (+6.8% versus +3.1%). More muscle growth was seen in the gluteus maximus, semimembranosus, semitendinosus and the biceps’ femoris long head.
To summarize, while the sub-group analysis in Figure 1 was certainly exploratory and preliminary, more consistent, positive data has been published since, increasing our confidence in the finding that lengthened partials could be/are better for muscle growth than a full ROM. However, these findings do beg some questions. Why does the muscle length at which resistance training is performed influence hypertrophy outcomes? Why do lengthened partials potentially lead to more muscle growth than a full ROM?
Why might lengthened partials work better?
To figure out why lengthened partials are leading to more hypertrophy within these studies, we can look to the sub-group of studies on ROM and muscle growth that measure outcomes that may mechanistically influence muscle growth. Unfortunately, few studies generally do this, and for good reason: the equipment and facilities required (not to speak of the additional time investment) are expensive and rare. However, we do have two studies that measured acute, mechanistic outcomes stemming from different ROMs.
The first study on ROM to measure acute, mechanistic data alongside hypertrophy is a study by McMahon et al (2014). They compared performing lengthened partials to shortened partials in a program composed of a variety of quadriceps exercises.
The lengthened partials were performed from 90 to 40 degrees of knee flexion, whereas the shortened partials were performed from 50 to 0 degrees. In addition to measuring changes in vastus lateralis cross-sectional area at various sites, McMahon et al (1) also assessed changes in insulin-like growth-factor-1 (IGF-1) from pre- to post-intervention when IGF-1 was measured at rest. Compared to the shortened partials group, the lengthened partials group saw greater overall increases in vastus lateralis cross-sectional area, particularly at the distal site, but also saw a significantly greater increase in resting IGF-1 levels. Consequently, the authors hypothesized that an increase in IGF-1 could be partly responsible for the superior hypertrophy observed in the lengthened partials group.
Mechanistically, IGF-1-related signaling plays an important part in maintaining anabolic sensitivity and in skeletal muscle remodeling. Interestingly, IGF-1 is released following both protein intake, but also mechanical contraction of muscle fibers, such as takes place during resistance training. Indeed, IGF-1 response post-workout may also vary depending on several factors such as rest times used, volume, and how much muscle was trained (1).
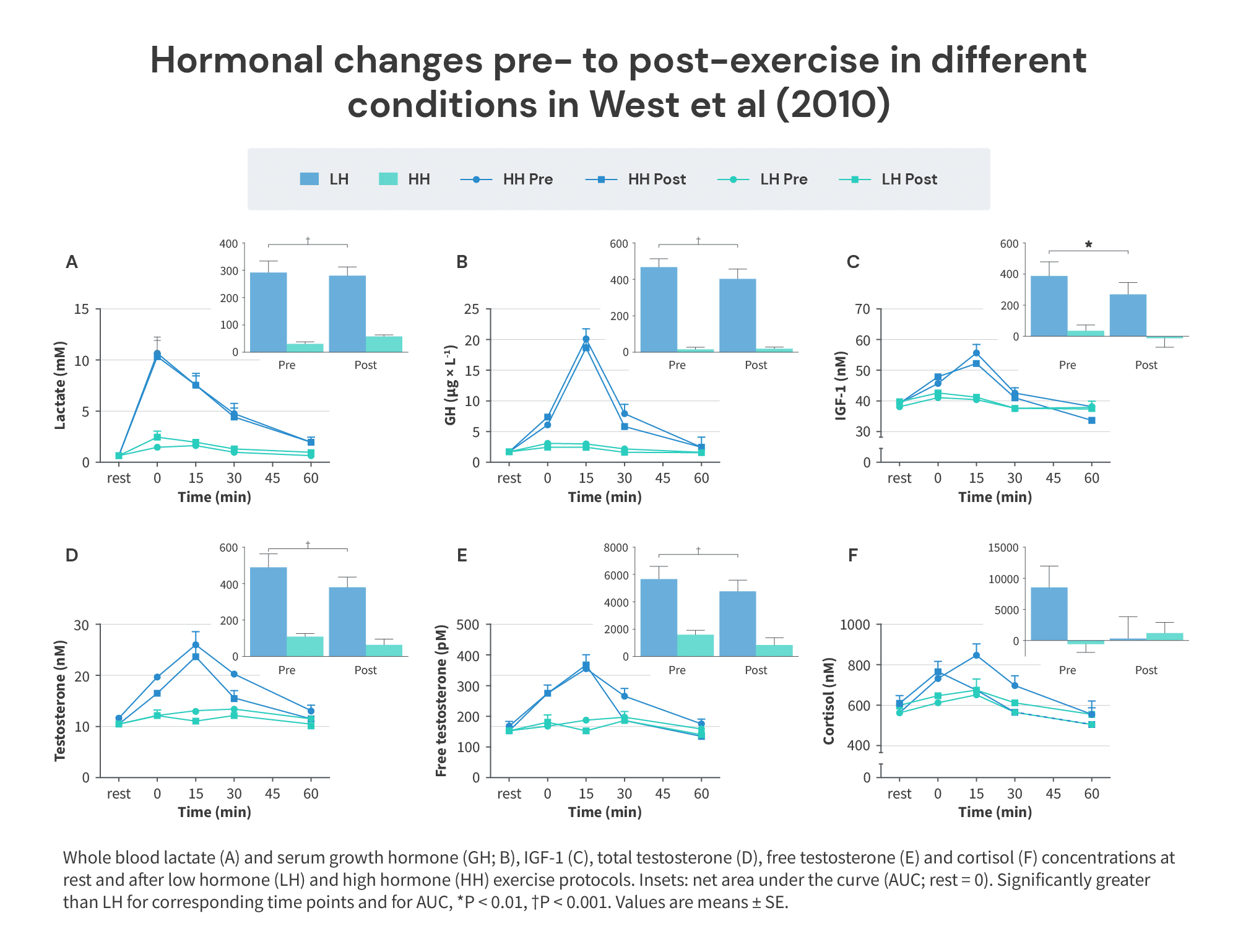
Yet, though IGF-1 is thought to impact hypertrophy-related signaling, most recent studies fail to find a connection between IGF-1 post-session and anabolic signaling (1, 2). Likewise, long-term, when it comes to muscle hypertrophy, IGF-1 has failed to be meaningfully associated with changes in muscle size. First, a study by Morton and colleagues (1) only found very weak correlations (r = -0.16 to 0.25) between acute increases in IGF-1 post-session and any measurement of muscle hypertrophy when participants trained using either a higher-rep (20-25 reps per set) or lower-rep (8-12 reps per set) protocol. Interestingly, in contrast to previous findings, with all sets taken to failure and number of sets equated for, increases in IGF-1 were similar between the lower- and higher-rep groups. Likewise, a study by West and colleagues (1) reported similar arm hypertrophy in a within-participant comparison of training one arm in a “high-hormone” milieu and the other in a “low-hormone” milieu. In the “low-hormone” condition, participants simply trained one of their arms with 3-4 sets of 8-12 reps of biceps curls close to failure. In the “high-hormone” condition, participants performed the same training with their other arm, but also performed 5 sets of 10 reps on the leg press and 3 supersets of 12 reps on the leg extension and leg curl, all close to failure, to elicit an acute hormonal response. Indeed, IGF-1 increased significantly more when also doing leg training (remember when it was commonly claimed that squats actually also grow your arms due to hormonal boosting?).
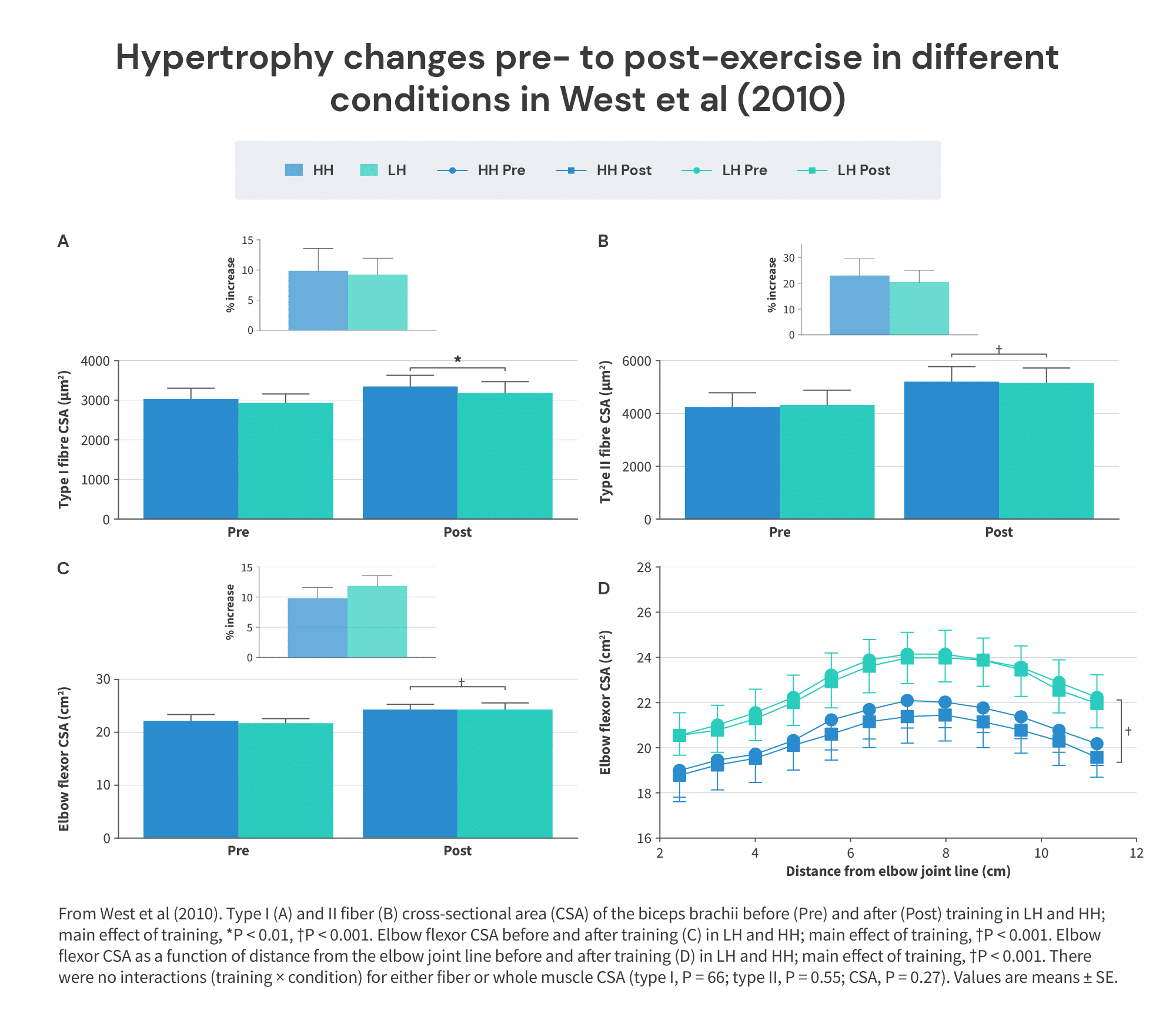
However, while IGF-1 did increase substantially more in the “high-hormone” condition, as intended, elbow flexor hypertrophy was nearly identical between groups.
So, what gives? Did the increase in IGF-1 from lengthened partials in the study by McMahon et al (2015) really contribute to greater hypertrophy or not?
In my opinion, probably not. If I had to hazard a couple of alternative explanations, here they are. First, it may have been the case that lengthened training generally stimulates greater increases in IGF-1 than shortened training, in the same way that shorter rest times, higher volumes, and larger muscles being trained can all increase IGF-1 increases. We know that muscle contraction initiates the IGF-1 response, after all. Importantly, although shorter rest times may increase IGF-1 production, they also blunt the hypertrophic potency of any given number of sets. Likewise, it may be the case that while lengthened training results in greater IGF-1 increases than shortened training, IGF-1 isn’t necessarily improving hypertrophy as a consequence.
Secondly, it may have been the case that the exercise selection within this study played a role in the IGF-1 response. The exercises performed (with the exception of the Sampson chair exercise) are generally hardest in the lengthened position and easier in the shortened position. You can probably quarter squat (0-50 degrees of knee flexion) a hell of a lot more weight than you can take reasonably close to parallel (0-90 degrees of knee flexion). Now, with that in mind, the participants in the shorter-muscle length group were essentially doing “quarter-squat-ROM” on all of their quad training, where the top of each rep could be considered quasi-rest. In contrast, the participants in the longer-muscle length group were cutting out the easy, top/lock-out part of the ROM altogether. If you’ve been lifting for a while, this may remind you of “constant tension training.” Just like shorter-rest times tend to increase IGF-1 release, cutting out the “intra-set rest” by skipping the lock-out could have a similar effect.
Importantly, in contrast with the study by McMahon et al (2015), both the study by West et al and Morton et al examined the post-exercise IGF-1 area under the curve – for around an hour – while McMahon et al looked at IGF-1 at rest. A superior increase in IGF-1 for only an hour post-exercise may be insufficient to induce meaningful differences in hypertrophy, whereas a longer-lasting increase, as noted by McMahon et al, may have been sufficient to cause differences in muscle hypertrophy. This explanation may or may not be a stretch (pun intended), but it’s worth noting. As a consequence, we likely shouldn’t dismiss IGF-1 as a potential mechanism altogether.
The second study that measured acute responses to different ROMs was a study by Goto and colleagues that was included in the sub-group analysis in Figure 1 (1). This study compared using a full ROM (from 120 degrees of elbow flexion to full extension) to partial ROM (from 90 degrees of elbow flexion to 45 degrees of elbow flexion) in the barbell skullcrusher exercise.
Feel free to skip this next paragraph if you’re happy to categorize this study as a lengthened partial versus full ROM comparison. If not, read on.
The comparison performed in this study can be difficult to categorize. On the one hand, the average joint angle in the partial ROM group (~67.5 degrees) was greater than in the full ROM group (~60 degrees), suggesting that, on average, the partial ROM group trained at longer-muscle lengths than the full ROM group. This is what resulted in the study’s inclusion as a comparison of lengthened partials and full ROM in the analysis in Figure 1. Equally, you could argue that 1) the difference in average joint angle/muscle length was minimal, 2) this was closer to a “mid-length” partial versus full ROM comparison, given how comparable the average joint angle was, and 3) a skullcrusher doesn’t fully lengthen the long head of the triceps brachii to begin with, making it a shortened partial versus full ROM comparison. I tend to sympathize with the first two perspectives. Amongst all the studies comparing lengthened partials to full ROM, this one walks the blurry line between “lengthened partial” and “mid-length partial” the most. With that being said, I do disagree with critique 3. First, very few comparisons actually involve training at the longest possible muscle lengths in any group. For instance, while many studies on the squat have “full ROM” groups, squat depth is usually curtailed well before participants reach their true full ROM (often between 90-140 degrees of knee flexion; 1, 2. Full knee flexion ROM is typically ≥150 degrees). Likewise, many of the comparisons of partial ROM at different muscle lengths involve biarticular muscles that are not being stretched to their fullest (1, 2, 3, 4). Therefore, to be logically consistent, the study by Goto and colleagues (1) wouldn’t even be a full ROM versus shortened partial comparison, since the long head is biarticular: it would be a partial ROM at short muscle lengths versus partial ROM at shorter muscle lengths comparison. Another issue arises when you consider that lengthening of a muscle does not occur uniformly throughout a ROM (1). More problematic still is the fact that we do not have measurements of fascicle lengthening of every muscle for every ROM in every exercise, which makes it somewhere between difficult and impossible to precisely categorize every ROM study in terms of the muscle lengths being trained through. Until we do have this data, I think it’s fair to (cautiously) compare conditions/groups within a study on the basis of a muscle’s functions and the average joint angles involved in the movements trained. To wrap this up, if one group trains at (on average) longer-muscle lengths than the other, and involves a sub-maximal ROM – as defined by the authors of the study – I would categorize it as “lengthened partials.” Just be aware that the details can get quite hazy, and how you classify this specific study is mostly a judgment call.
To return to the methods of Goto et al (2017), lifters with at least one year of training experience performed the skullcrusher three times per week for eight weeks. Both groups trained with the same volume and took every set to failure. Alongside assessing changes in estimated triceps cross-sectional area, Goto and colleagues also measured peripheral muscle oxygenation and blood lactate concentration at rest, immediately after, and five minutes after performing the full ROM and lengthened partial protocol. The authors also assessed triceps activation during the full ROM and lengthened partial protocols, scaled to activation measured during a maximal voluntary contraction. These acute measurements were repeated both before and following the eight-week training intervention. Increases in estimated triceps brachii cross-sectional area were larger in the lengthened partial group (+48.7%) than the full ROM group (+28.2%). Acutely, the lengthened partial protocol led to larger increases in blood lactate concentration, deoxygenation of the triceps, and triceps EMG than the full ROM protocol. While these acute responses could reveal some insights into the mechanistic underpinnings of LPs, the effects of blood lactate, muscular hypoxia, and motor unit activation on muscle hypertrophy remain contentious.
Muscular hypoxia has been hypothesized to increase the hypertrophy stimulus of lifting weights through greater accumulation of metabolic byproducts, such as the aforementioned lactate. Therefore, muscular hypoxia can be considered a (potentially) indirect hypertrophy stimulus rather than a mechanism directly increasing anabolism. Importantly, by increasing accumulation of metabolite byproducts, intentionally inducing hypoxia reduces performance in the gym, which may or may not be desirable. Regardless, the most recent meta-analysis (1) comparing lifting in a normoxic (normal oxygen availability) to a hypoxic (lower oxygen availability) environment found little, if any, benefit to lifting in a hypoxic environment for muscle growth (SMDs range from -0.06 to 0.17). Importantly, there were relatively few studies measuring hypertrophy as an outcome, and training protocols varied substantially. Similarly, on a local level, training with low loads and using blood flow restriction generally doesn’t cause greater muscle hypertrophy than normal high load training (1). This is notable, since low-load blood flow restricted training generally causes greater muscle deoxygenation (1). Overall, it’s unlikely hypoxia is directly responsible for greater hypertrophy from lengthened training, but it’s possible that lengthened training generally results in greater muscular hypoxia, thereby leading to greater metabolite accumulation, possibly resulting in an additive effect on muscle hypertrophy.
On the one hand, exogenous lactate administration has been shown to increase anabolic signaling and reduce muscle atrophy during a calorie deficit in rodents (1). However, a subsequent study by the same authors examined muscle hypertrophy in rodents when lactate was administered alongside two mechanical overload protocols of varying intensities (2). In this study, when combined with mechanical overload – which can be seen as a form of resistance training, mechanistically – lactate administration failed to increase the degree of muscle hypertrophy or anabolic signaling observed. Together, these studies suggest that while lactate may play a role in stimulating hypertrophy, it may not have an additive effect when you’re also exposing your muscles to tension through resistance training. Importantly, whether this relationship generalizes to humans remains unclear (1). For example, a study by Liegnell et al (1) performed intravenous infusion of lactate in humans and measured anabolic signaling, failing to find a meaningful effect on mTOR and ERK pathway activity. Therefore, while lactate could play a role in the muscle hypertrophy response from lengthened training in humans, it remains unclear whether lactate’s effect on hypertrophy is additive to tension-mediated hypertrophy.
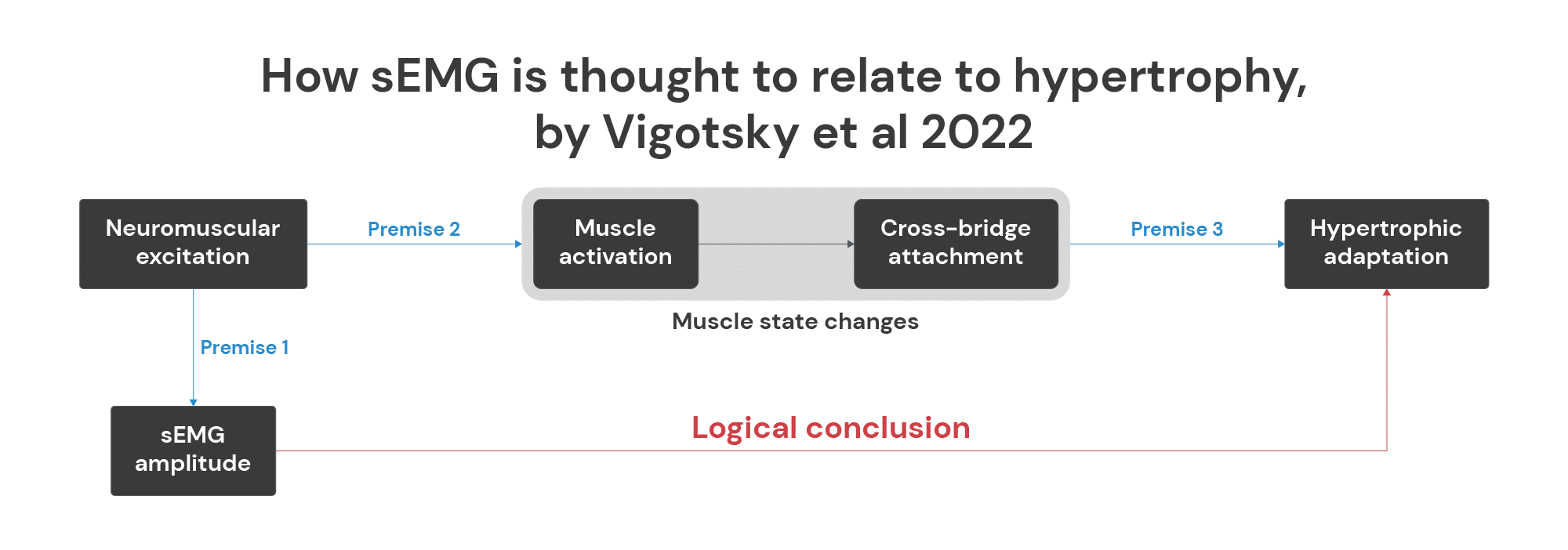
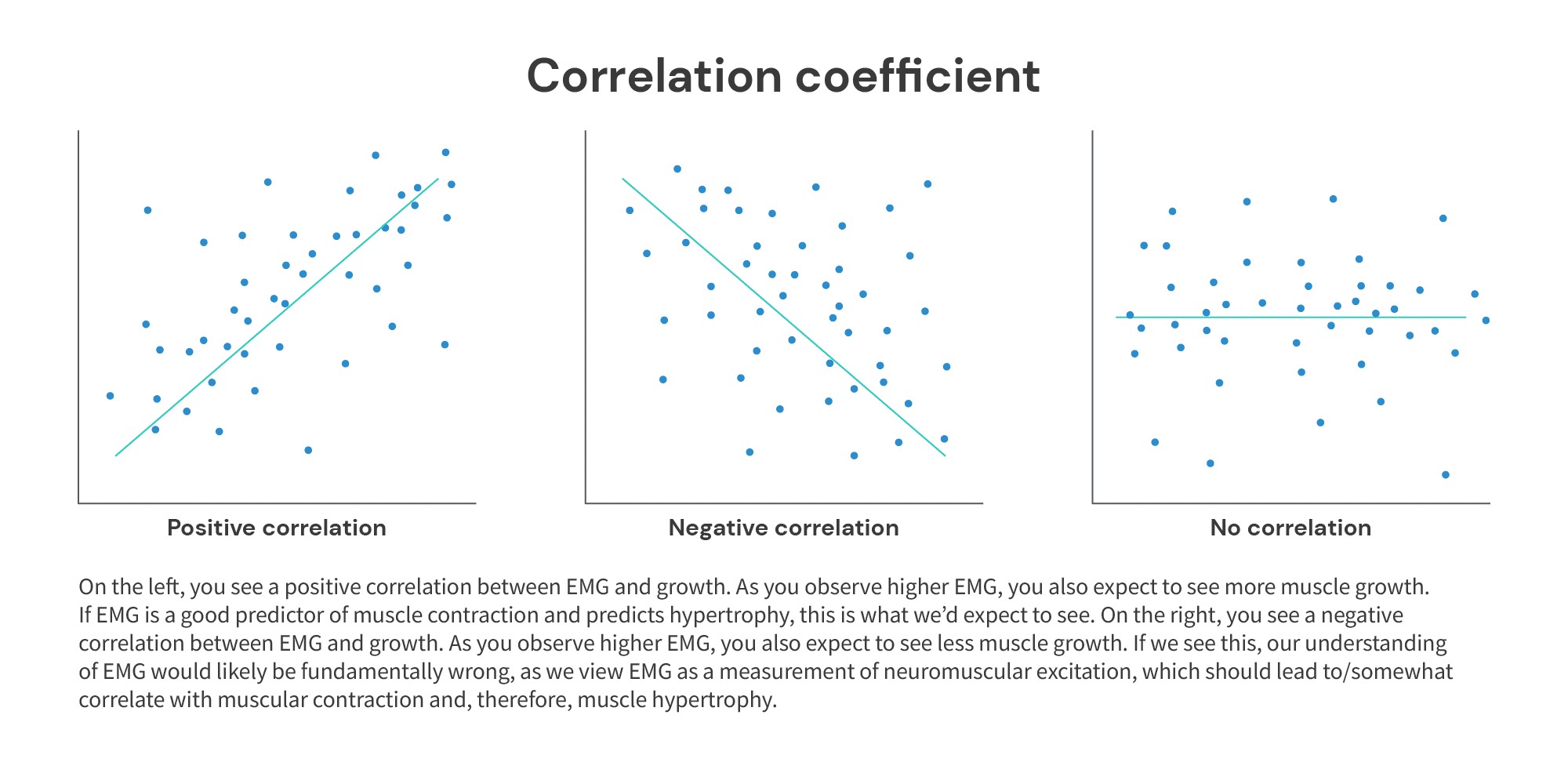
Muscle activation is commonly measured using surface electromyography (EMG), as was done in the aforementioned study by Goto and colleagues (1). Mechanistically, greater EMG reflects neuromuscular excitation, which is the signal that eventually leads to a muscle being activated. Following activation, cross-bridging of actin and myosin occurs, leading to muscle contraction. Therefore, the magnitude of EMG observed is often assumed to be a good predictor of the degree to which a muscle contracts. However, as Vigotsky and colleagues (1) have pointed out, these links remain largely unsubstantiated (see Figure 5 below). While surface EMG does measure neuromuscular excitation, the degree to which EMG correlates with muscle activation, cross-bridging of actin and myosin/muscular contraction, and long-term muscle growth remains a big gap in the literature.
Putting aside these theoretical gaps that we would need to address before we can rationalize EMG as something that should predict muscle growth well, the observed validity and reliability of EMG as a predictor of muscle hypertrophy also remain questionable. For example, a study by Plotkin et al (1) compared the hip thrust to the squat exercise. The authors first measured EMG in a variety of areas of the glutes, including the upper, mid, and lower gluteus maximus and the gluteus medius during the squat and hip thrust exercise. Then, participants were randomized into a group performing either just squats or just hip thrusts for nine weeks. The authors measured muscle growth of different muscles using MRI from before to after the nine-week training program, including the glutes. Alongside seeing which exercise led to more muscle growth, the authors also conducted an analysis to see whether the EMG results from before the study were associated with regional muscle hypertrophy of the glute musculature. They did so in three different ways:
- Between-subjects (did subjects who saw greater glute EMG readings also grow more?).
- Between-regions (did areas of the glutes that saw greater EMG also grow more?).
- Between-exercises (did the exercise that resulted in greater EMG also cause more growth?).
In the context of the Goto study (1), analysis 1 is most relevant, as the site of measurement for muscle growth was the same (making analysis 2 irrelevant) and both groups performed the same exercise (the skullcrusher), making analysis 3 irrelevant. To cut to the chase, none of the analyses panned out. No matter the exact way EMG’s predictive ability was tested, EMG was – at best – a weak and inconsistent predictor of muscle hypertrophy. In the context of the Goto study, analysis 1 resulted in correlations of r = -0.03 to 0.5 between EMG and muscle growth in the glutes between subjects. Fortunately, the associations were positive, meaning that at the very least, greater EMG means “somewhat” more muscle growth, not less (as we’d expect with negative correlations).
All in all, the human research on lengthened training tells us remarkably little about which mechanisms might contribute to greater hypertrophy stemming from lengthened training. To be sure, there are other potential mechanisms that come up in conversations about this topic (which we discussed at length in a prior article), but they must be regarded as even more speculative, since there’s no direct human evidence demonstrating that they contribute to the hypertrophy response observed with lengthened training. To summarize:
- Lengthened partials could lead to greater muscle deoxygenation, blood lactate increases, muscle activation, and/or IGF-1 increase during training compared to more shortened training (e.g. full ROM). However, the above remains to be firmly established as we are drawing on only two studies.
- Assuming the above does hold true, these mechanisms could contribute to greater muscle growth from lengthened training. Muscle hypoxia, lactate, muscle activation, and IGF-1 can all theoretically impact downstream anabolism and therefore muscle hypertrophy. However, studies directly measuring the relationship between these physiological variables and muscle hypertrophy in humans performing resistance training are sparse and correlations are generally weak-to-moderate at best (in the range of r = -0.16 to r = 0.5), explaining about ~2.5 to 25% of covariation in muscle growth.
- In light of how weak the correlations above are, it is tempting to disregard these mechanistic findings altogether. However, it is important to remember the magnitude of additional hypertrophy we expect to see with lengthened partials versus full ROM (+6.76% growth versus full ROM). With a difference in hypertrophy as small as this one, it is entirely plausible that a mechanism with a similarly modest impact on skeletal muscle hypertrophy could be responsible.
…so, does that take us back to square one, or is there other data that could help explain why training in the lengthened position is beneficial for muscle hypertrophy? Since the only difference between lengthened training and shortened training is how much of your training takes place in the stretched position, is there something special about the stretch?
What is stretch-mediated hypertrophy?
Stretch-mediated hypertrophy (SMH) is muscle hypertrophy occurring as a result of stretching, or lengthening, of sarcomeres.
Research into SMH has been ongoing since the 70s and had its start in animal models. Animal studies have distinct advantages. Specifically, it can be easier to conduct “proof-of-principle” studies with extreme protocols designed to elicit an observable, measurable effect when we’ve identified a specific mechanism or suspect an effect exists. Similarly, hypertrophy can be more easily/precisely measured, as the unfortunate practice of sacrificing research animals remains common.
A classic example of such a study was conducted by Sola and colleagues in 1973 (1). 100g and 200g weights were attached to the wings of chickens to induce stretch-mediated hypertrophy of latissimus dorsi and teres minor muscles, with the other wing serving as a control group. Dramatic hypertrophy of the lat muscle being stretched was observed, with an increase in muscle weight of up to ~170% being observed. Importantly, Sola examined muscle hypertrophy resulting from this stretching intervention in both innervated and denervated muscles (i.e. supplied with nerves or not). Since only innervated muscle can actively contract, this study provides an estimate of how much hypertrophy is truly stretch-mediated versus mediated by active contraction under load. Indeed, while many studies measure stretch-mediated hypertrophy, these measurements also include non stretch-mediated hypertrophy, since the muscles are also actively contracting. Sola et al found that the denervated muscles increased in weight by ~140%, whereas the innervated muscles’ weight increased by around ~170%. This suggests that most of the hypertrophy observed was truly stretch-mediated, as even denervated muscles experienced an increase in muscle weight of ~140%. Conversely, the remaining 30% may have been attributable to active contraction. Truly “stretch-mediated hypertrophy” can occur with both innervated and denervated muscles – this distinction is important.
This study by Sola is not the only one that has been conducted on the topic of SMH in animals; there have been dozens of studies in the same vein. The results of these studies were recently summarized in a meta-analysis by Warneke et al (1). 16 animal studies that included at least 15 minutes of stretching per day were analyzed. As you’d expect based on the results by Sola and colleagues (1), stretching interventions resulted in drastically greater increases in muscle mass compared to a control condition (d = 8.51, 95% CI 7.11- 9.91). For context, in humans just lifting weights, compared to a non-training control group, we typically observe muscle growth around d = 0.34 (95% CI 0.29 – 0.39), with some variance depending on the exact study (1). In other words, there’s comfortably an order of magnitude of difference between the hypertrophy observed in typical resistance training studies performed in humans and these stretching studies in animals. Indeed, extreme increases in muscle mass of up to 200 to 300% of initial muscle mass in less than six weeks aren’t unheard of in this body of evidence.
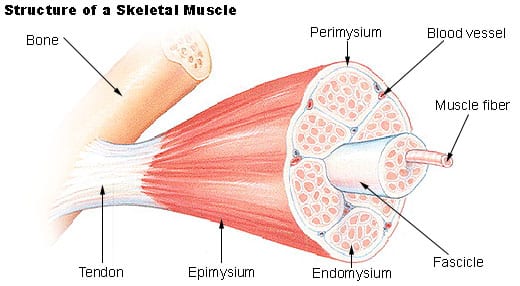
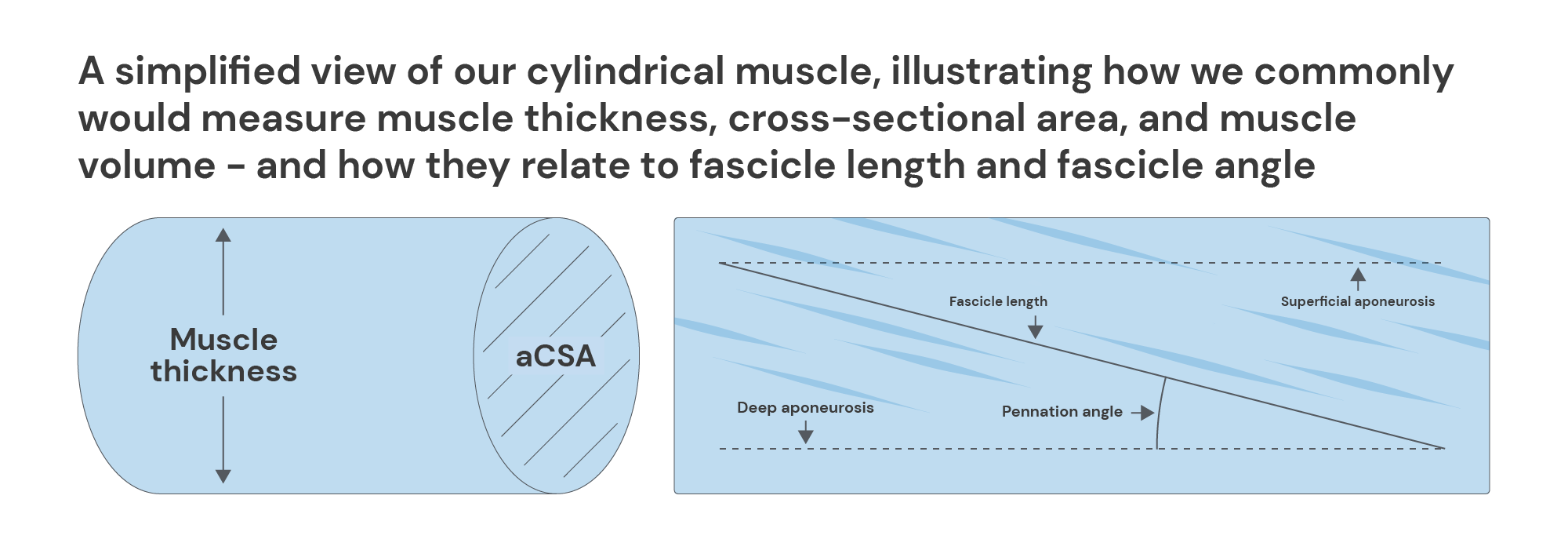
In order to fully understand these results, let’s review a primer on how muscle grows. Human muscle growth is thought to (mostly) occur when existing muscle fibers (or myofibrils) increase in size. Muscle fibers themselves are composed of smaller, functional units called sarcomeres. Though muscles vary in shapes, it’s easiest to visualise a muscle as a cylinder when conceptualising its growth.
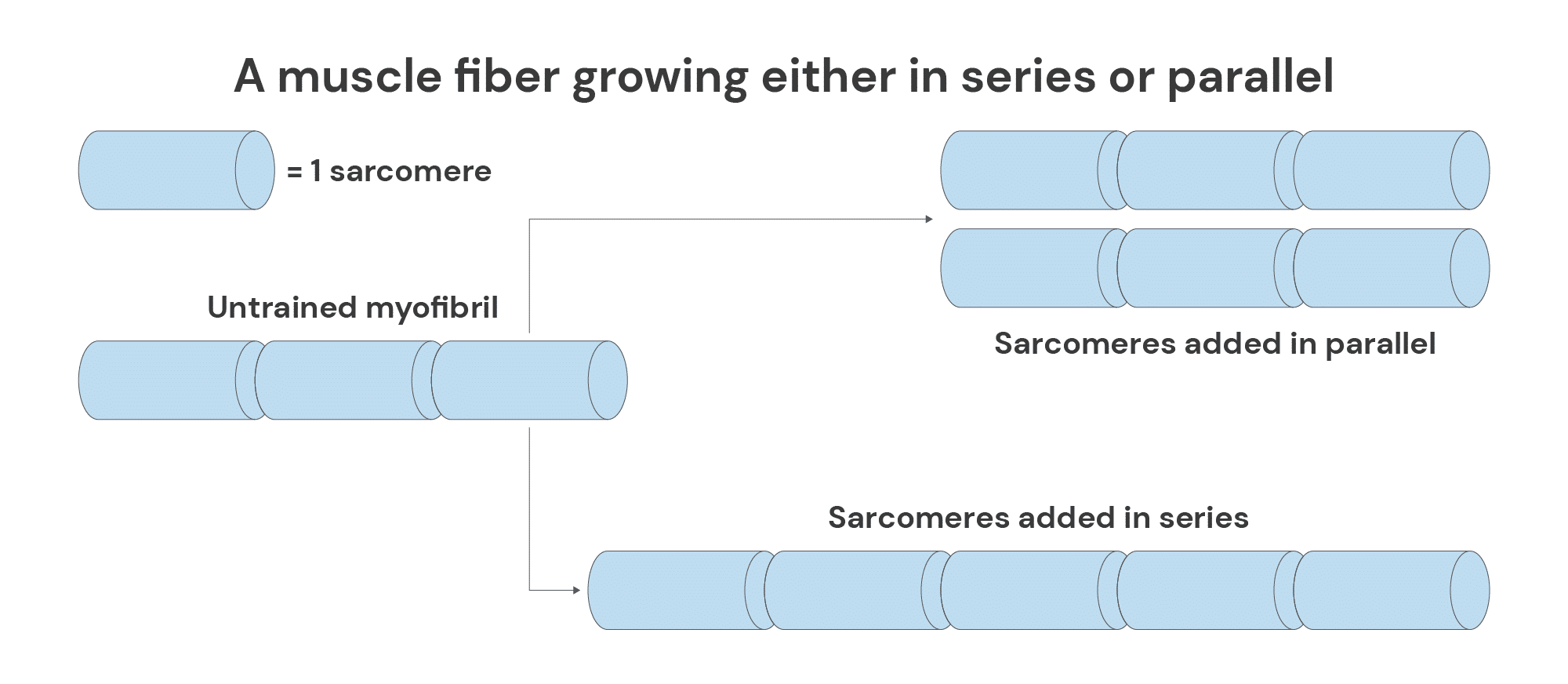
When a muscle grows in size, this can occur either radially/“in parallel” or longitudinally/“in series.” Radial hypertrophy occurs through the addition of sarcomeres in parallel. Conversely, longitudinal muscle growth occurs through either the addition of sarcomeres in series or through the increase in length of individual sarcomeres, leading to increased myofibrillar length.
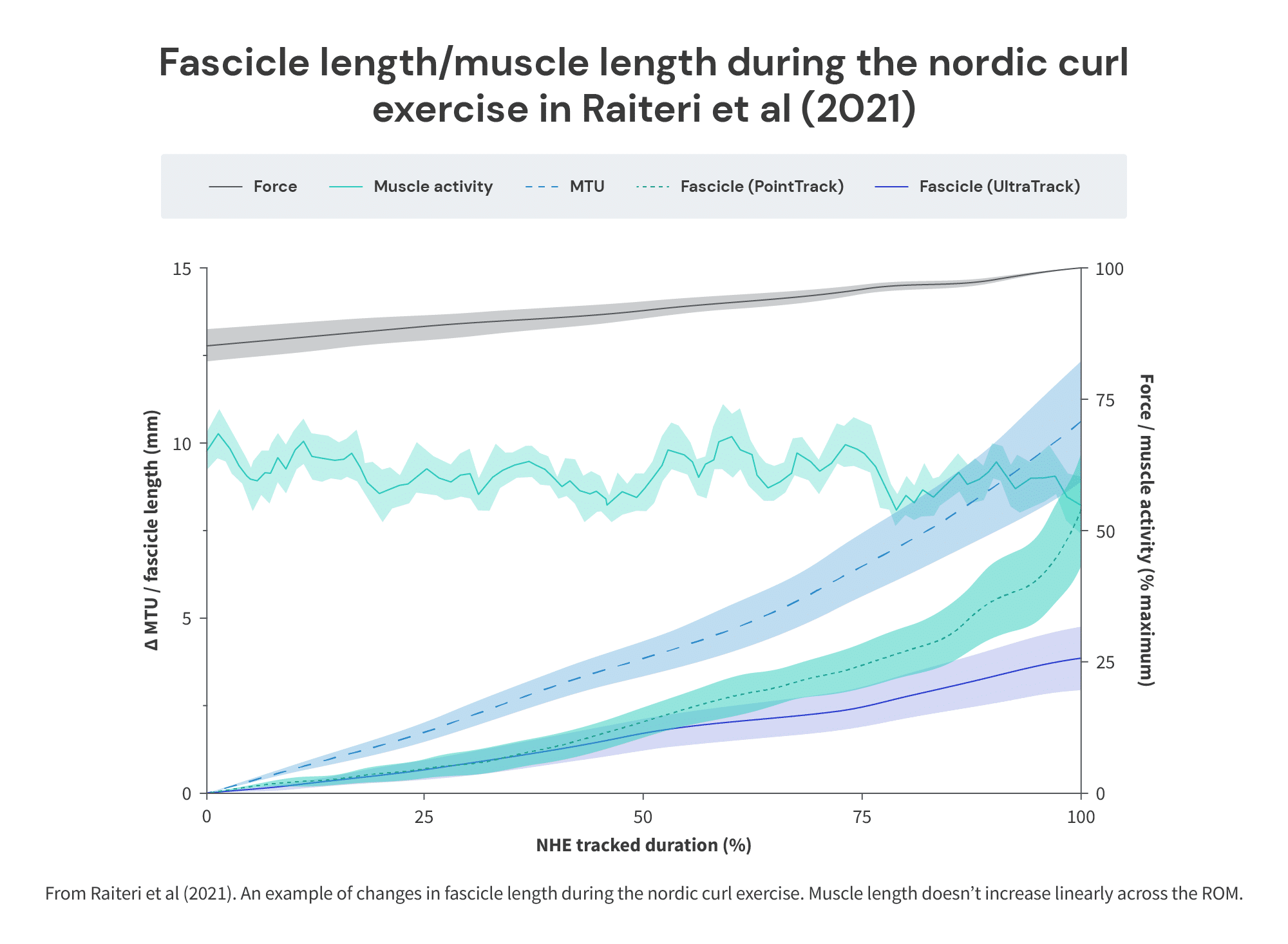
Importantly, increases in pennation/fascicle angle are generally thought to reflect increases in radial hypertrophy, whereas increases in muscle fiber/fascicle length are generally thought to reflect increases in longitudinal hypertrophy.
With that primer done, let’s return to the results of the meta-analysis by Warneke et al. The authors also analyzed the addition of new muscle fibers (also called “hyperplasia”) and increases in fiber length, which represent longitudinal hypertrophy. Substantially greater hyperplasia was observed in the stretching condition of most of the studies included, suggesting new muscle fibers do get created in response to stretching in animals (d = 4.62, 95% CI 2.54-6.71). With regards to longitudinal hypertrophy, only three studies measured fiber length. That said, across those three studies, substantially greater increases in fiber length were also observed in the stretching condition compared to the control condition (d = 7.86, 95% CI 4 – 11.72; or, in % changes, +26.1%).
To summarize, the concept of SMH first originated from studies of long-duration, daily, static stretching in animal models. Adaptations to such interventions have been coined stretch-mediated hypertrophy and are characterized by:
- A very drastic increase in muscle mass.
- A notable magnitude of myofibrillar hyperplasia, or addition of new muscle fibers.
- An increase in fiber length/longitudinal hypertrophy.
So, dramatic hypertrophy absolutely appears to be a consistent phenomenon when animals are exposed to stretching interventions. Does this also apply to humans? Do we observe a similar phenomenon when humans are exposed to stretching interventions?
Transferability from animal stretching to human stretching research
Muscle Hypertrophy
The literature examining muscle growth in response to stretching interventions in humans was most recently summarized in a narrative review by Warneke et al (1). In total, though this was not a systematic search for all studies on the topic, ten studies were found. To give you a brief lay of the land, four of ten studies found no significant improvements in muscle size. Conversely, the remaining six studies observed some hypertrophy in response to stretching, with increases in muscle size ranging from ~5 to 25% over 5 to 12 weeks. Notably, this body of evidence was also meta-analyzed recently by Panidi et al (1).
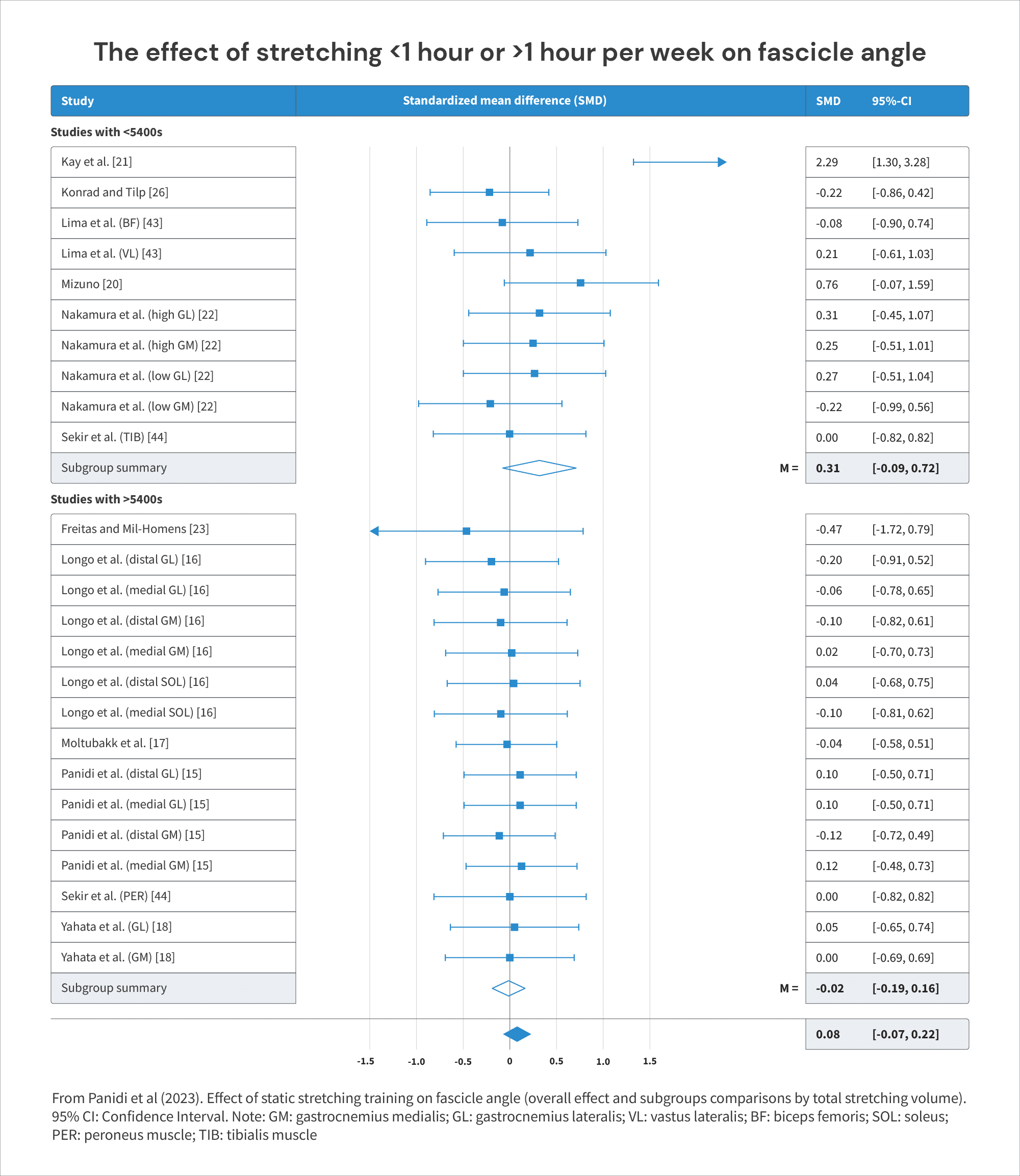
Stretching interventions generally had very little, if any, impact on increases in pennation angle (SMD = -0.02 – 0.15). That said, increasing the volume of stretching to more than 1.5 hours of stretching per week appeared to increase the effect appreciably (SMD = 0.32, 95%CI -0.09 0.72). These findings suggest stretching has a minimal impact on increases in radial hypertrophy, at least when volumes are relatively modest.
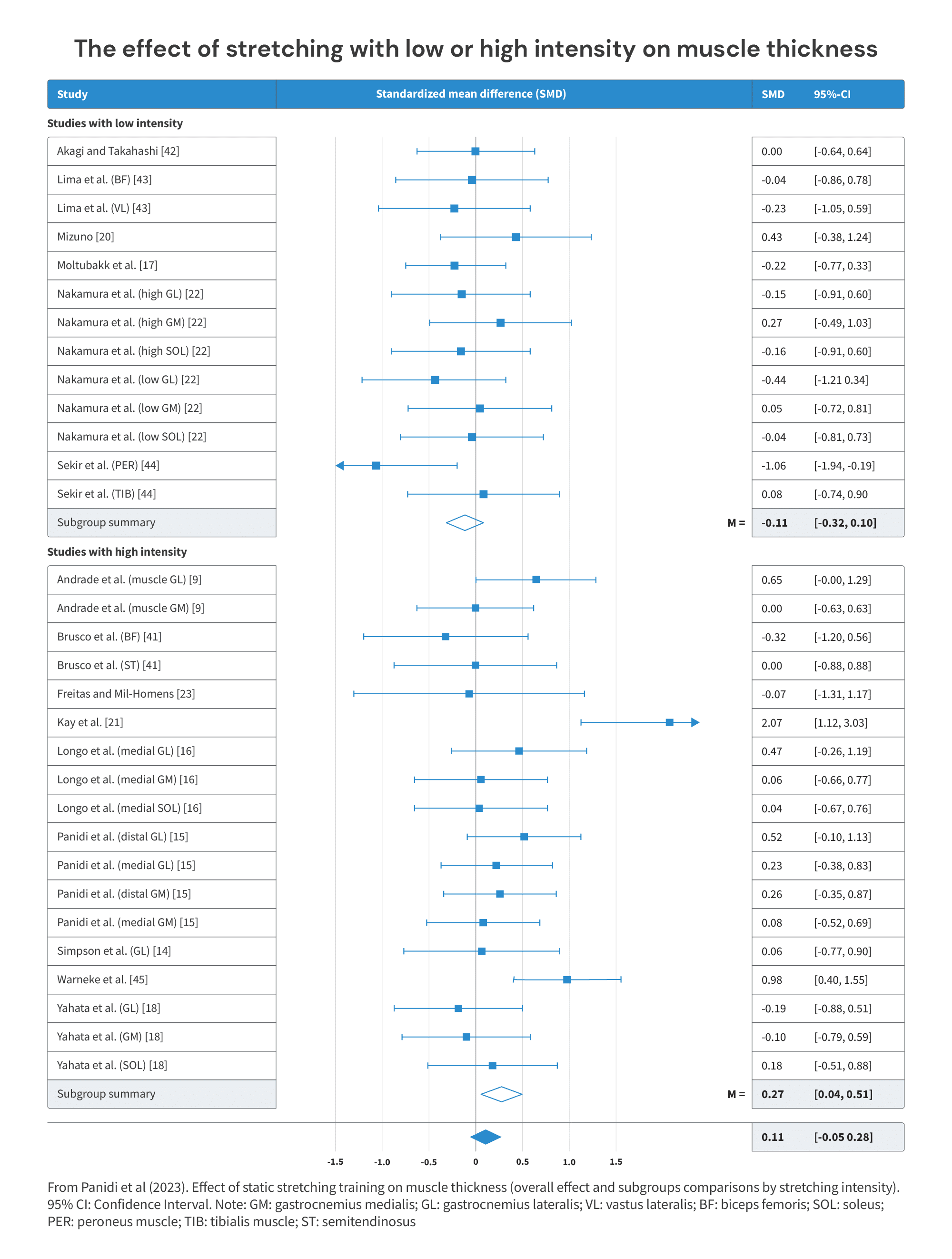
With regards to direct measurements of muscle hypertrophy, stretching interventions had next to no effect on muscle thickness when all studies were included in the analysis (SMD = 0.11, 95% CI -0.05 – 0.28). Likewise, when grouping studies by volume and whether the stretching intervention lasted less or more than 1.5 hours/week, neither shorter nor longer protocols substantially increased muscle thickness (SMD = 0.11 and SMD = 0.13, respectively). In contrast, when grouping studies by the intensity of the stretching protocol, high intensity stretching did cause notably more hypertrophy compared to low intensity stretching (SMD = 0.27 versus SMD = -0.11). Overall, changes in muscle thickness were lower than we generally observe from lifting weights, though higher intensity stretching may slightly increase the muscle hypertrophy induced by stretching.
This represents the first significant limitation in transferability from the animal stretching data to human physiology. Despite greater intervention durations (5-12 weeks versus <6 weeks), the hypertrophy observed is of a much smaller magnitude (d = 0.11 – 0.27 based on Panidi et al or ~5-25% in human studies that do detect hypertrophy based on Warneke et al 2023 versus ~1-300% in animal studies). Some of this could be chalked up to differences in the duration and intensity of stretching performed; the longer and more intense stretching bouts may generally lead to greater hypertrophy, both through increases in fascicle length, and, potentially, pennation angle (1, 2).
Notably, animal studies generally employ stretching protocols that are longer in duration and impose greater tension, potentially explaining the drastic difference in hypertrophy observed. That said, the gap in duration of stretching does not fully explain the disparity in hypertrophy observed, as a series of studies by Warneke (1, 2, 3) with 60 minutes of daily stretching only observed increases in muscle size of 4.68 to 8.8% over six weeks. A six-week animal study by Frankeny and colleagues (1) measured increases in muscle cross-sectional area of chickens in response to stretching with a variety of durations (24 vs. 8 vs. 4 versus 2 vs. 1 vs. 0.5 hours per day). The increases in muscle size observed were drastically larger than those observed by Warneke and colleagues in the three aforementioned studies (68.8% in Frankeny vs. 4.68 to 8.8% in the three studies by Warneke).
However, it is possible that differences in the tension imposed upon the muscle during stretching is responsible for differences in adaptation. While methods vary, one common method in animal models is to stretch the target muscle with ~10-12% of the animal’s body weight. In contrast, in human studies, prescribing and standardizing tension applied is challenging. Generally, stretching boards or orthoses are used to apply the stretch intervention in human participants.

In the aforementioned series of studies performed by Warneke and colleagues (1, 2, 3), for example, an orthosis was used to apply a stretch for an hour daily on the gastrocnemius/calf muscle for six weeks. Participants were instructed to keep their knees fully extended and reach a maximally dorsiflexed position with a “stretching pain” score of 7-8 out of 10 on a visual analog scale. The orthosis was then set and the stretch was maintained for one to two hours daily.
To further muddy the waters, some research (1) suggests that, during stretching, pain ratings on a visual analog scale, as were used by Warneke and colleagues, show essentially no correlation with tension applied (ρ = -0.084, p = 0.497). Ultimately, it is virtually impossible to try to compare the intensity of stretch used in the animal literature to the intensity of stretch used in the human literature and attempt to draw conclusions.
Fiber number/hyperplasia
While humans do likely experience myofibrillar hyperplasia, as multiple indirect lines of evidence suggest (1), no studies currently exist on myofibrillar hyperplasia in response to stretching interventions in humans. Therefore, it remains unclear whether stretching has the potential to elicit this adaptation in humans versus animals.
Fiber length
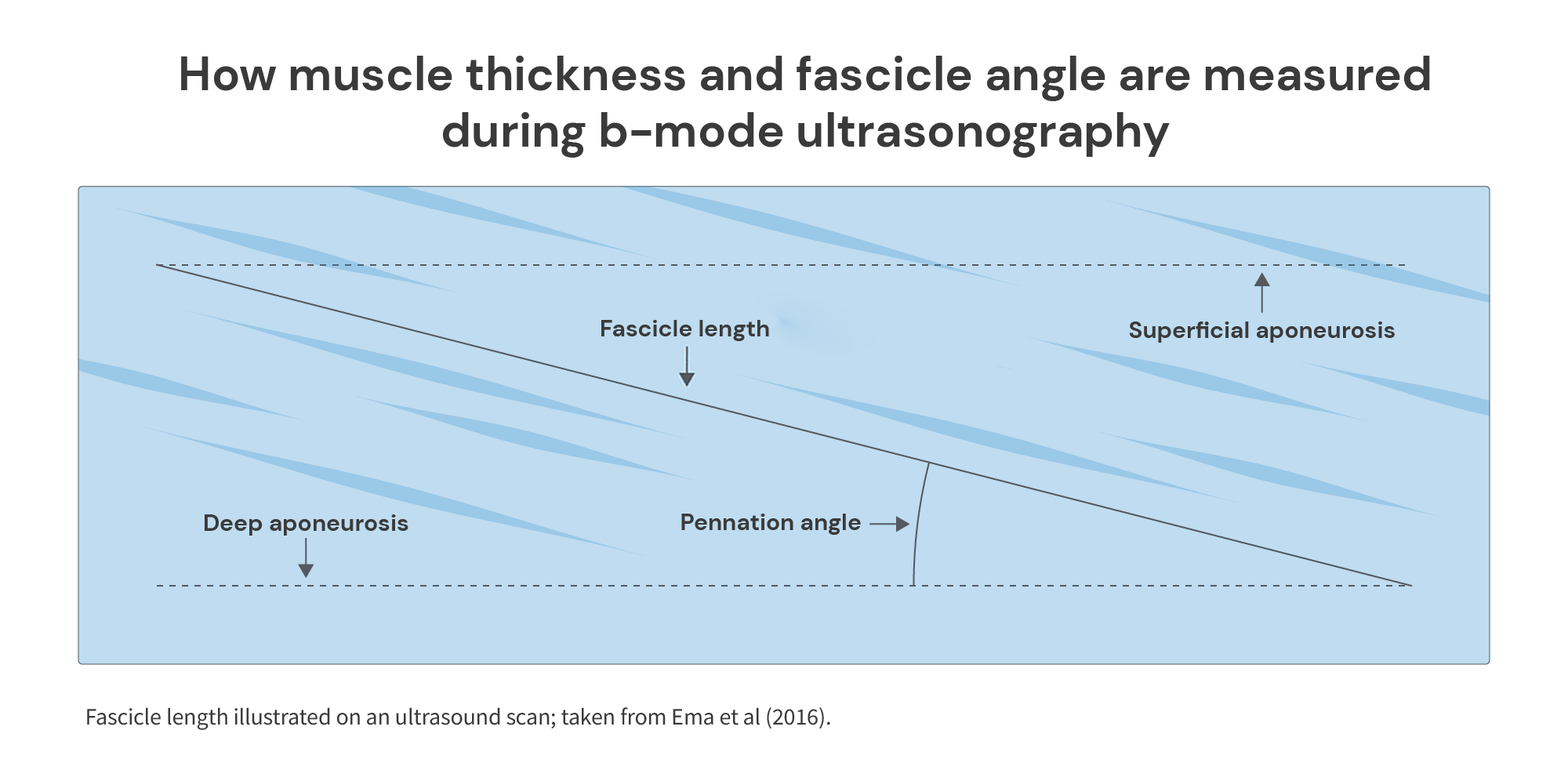
Fiber length is rarely directly measured within stretching intervention studies. They are small and difficult to measure individually (1). However, an indirect measurement of fiber length is often taken: fascicle length. Muscle fascicles are essentially bundles of muscle fibers that all share a similar orientation.
In animal studies, muscle fiber length is often assessed by sacrificing and dissecting lab animals. Unfortunately/fortunately, the same isn’t being done for humans. Instead, we need to be a bit more creative. Using ultrasound technology, we can assess the length of these fascicles, which is assumed to serve as a proxy for muscle fiber length. There are various methods to assess/estimate fascicle length, from using extended-field-of-view ultrasound, which allows you to visualize the whole fascicle and more accurately measure its length, to estimating its length using trigonometry after visualizing a section of the muscle (this is referred to as “linear extrapolation”).
The aforementioned meta-analysis by Panidi et al (1) also reviewed the data on increases in fascicle length in response to stretching interventions in humans. When all studies were included in the analysis – 14 in total – stretching interventions resulted in a very minor increase in resting fascicle length compared to a control condition (SMD = 0.17, 95% CI 0.01-0.33). That said, the effect became slightly larger when exclusively analyzing longer duration stretching protocols (more than 1.5 hours of stretching per week) and stretching protocols with higher intensities (SMD = 0.28-0.29), suggesting that volume and intensity do impact the degree of adaptation observed. Regardless, the magnitude of adaptation in fascicle length remains relatively modest, particularly when contrasted to the magnitude of adaptation in fiber length observed in animal models. While only three studies were included in the analysis on fiber length in the aforementioned meta-analysis by Warneke et al (1), the SMD observed was much larger in animal studies compared to the presently reviewed human studies (SMD = 7.86 versus SMD = 0.17-0.29).
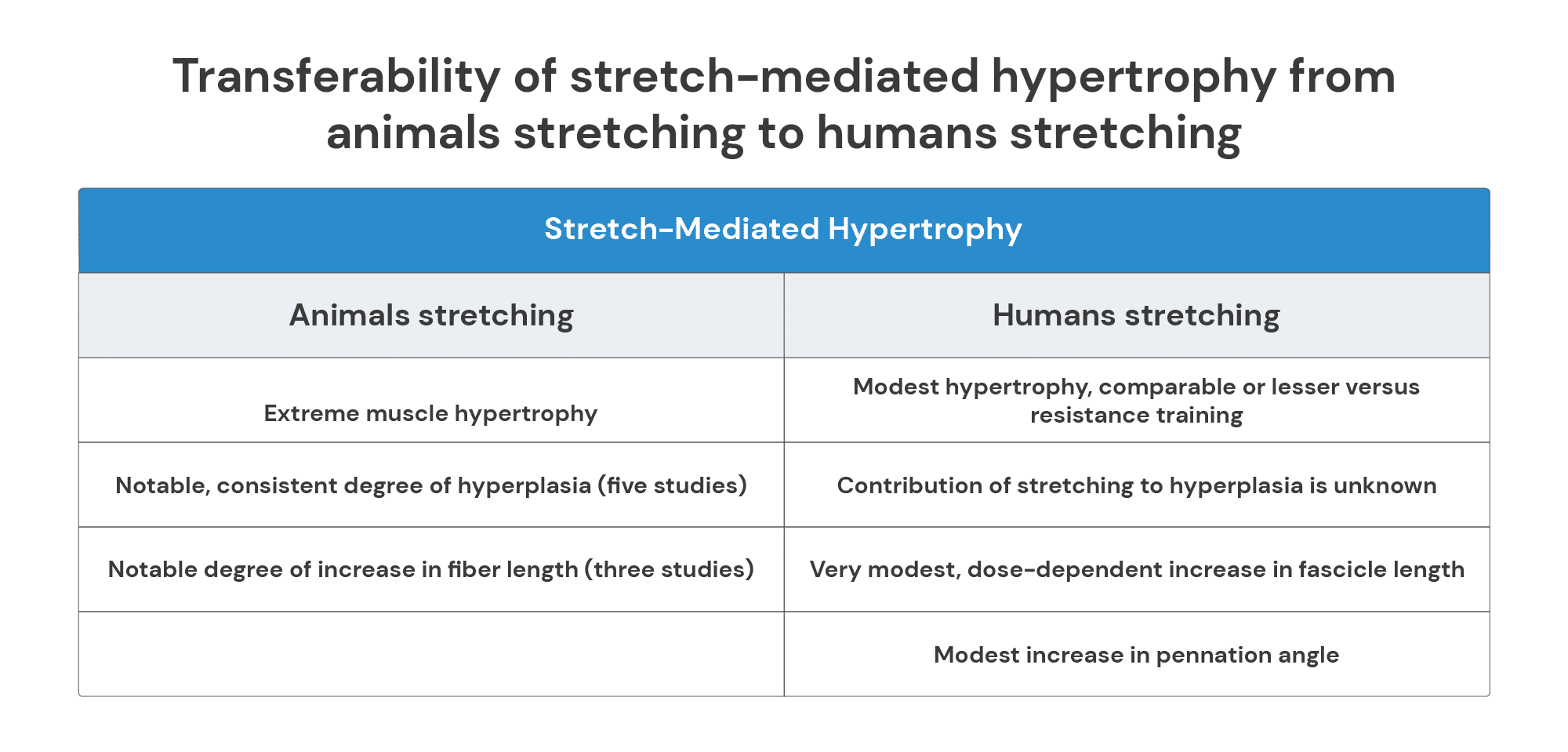
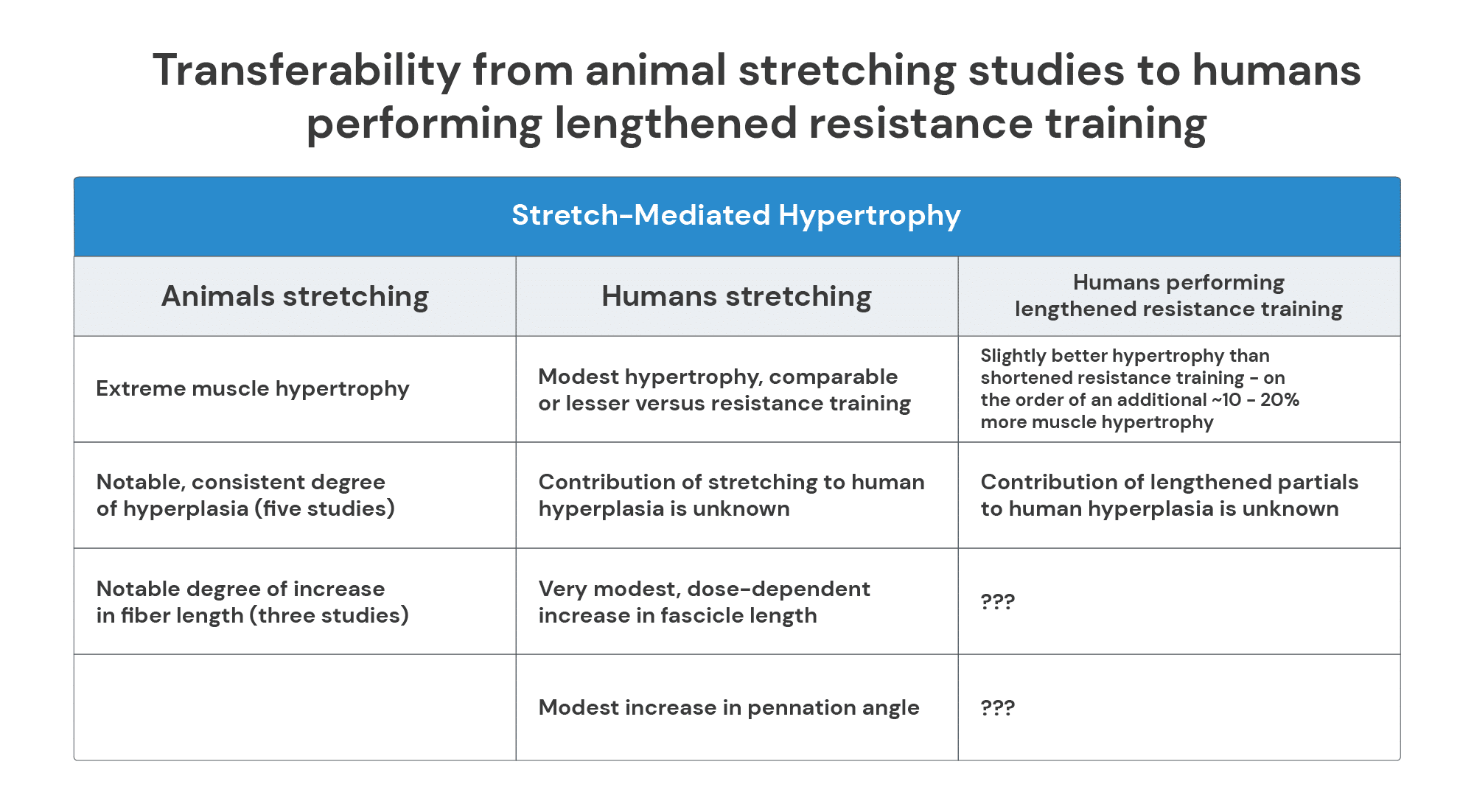
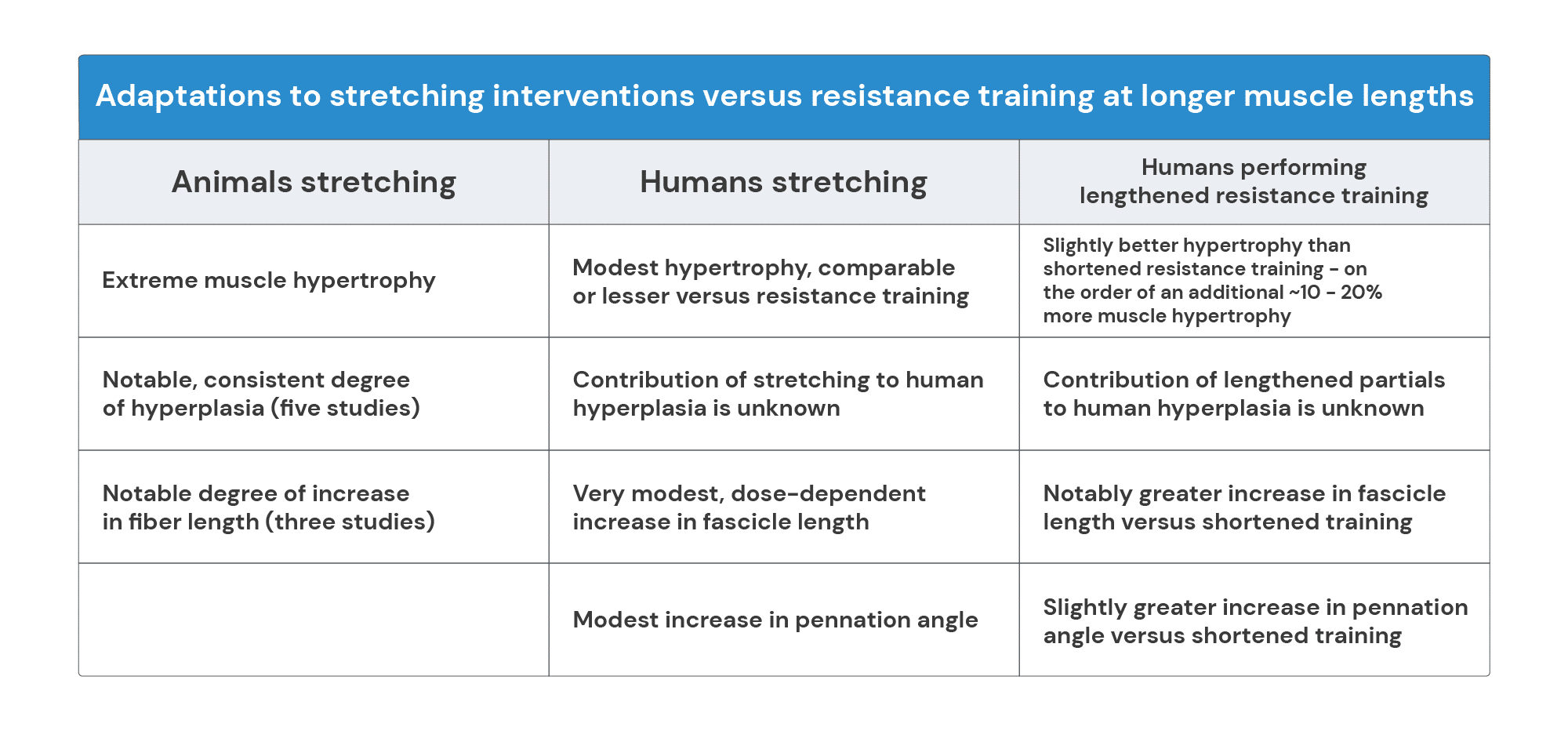
Table 3. Transferability of stretch-mediated hypertrophy from animals stretching to humans stretching.
Overall, the effects of SMH on muscle size are much more modest in humans than in animals, and the degree of hyperplasia remains unknown. These differences may be the result of humans and other animals responding to stretch differently, or they may simply be a result of the stretching interventions used (i.e., up to an hour of stretching per day in humans versus 24/7 stretching for several weeks in animals). There appears to be some transferability/congruence between the effects of stretching interventions in animals versus humans, but it is of limited scope and magnitude.
Importantly, this already casts doubt on the idea that lengthened partials are stimulating “stretch-mediated hypertrophy.” If notable improvements in muscle size, fascicle length, and pennation angle are only observed at higher durations (more than an hour of stretching per week) and intensities, it seems unlikely that spending a few extra seconds per workout at longer-muscle lengths would be sufficient to induce “stretch-mediated hypertrophy” during lengthened partials or any other modality emphasizing the lengthened position.
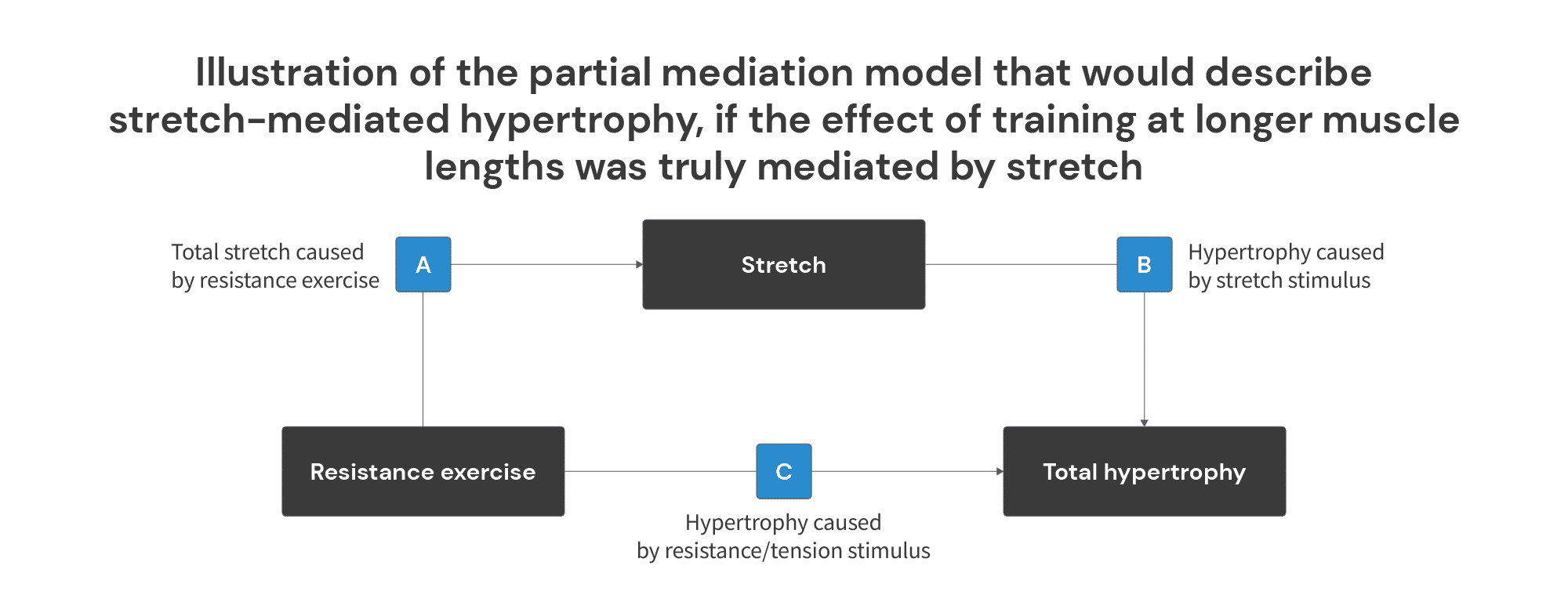
In other words, if stretch is truly mediating the effect (i.e. if we’re truly dealing with “stretch-mediated hypertrophy”), the difference between hypertrophy observed when training at long muscle lengths and hypertrophy observed when training at short muscle lengths should be directly attributable to the actual stretch that occurs when training at long muscle lengths. So, total hypertrophy would be equivalent to the hypertrophy caused by the “normal” tension stimulus that comes from resistance training, plus the hypertrophy caused by the stretch experienced when training at longer muscle lengths.
With this in mind, it should be clear that most (probably all) of the studies demonstrating increased muscle growth when training at longer muscle lengths aren’t demonstrating stretch-mediated hypertrophy, because none of the training interventions in these studies would produce a sufficient stretch stimulus to independently cause robust hypertrophy, and most wouldn’t produce any significant stretch stimulus at all.
To illustrate, Pedrosa and colleagues observed approximately twice as much quad hypertrophy when training knee extensions through a range of 65-100° of knee flexion versus 30-65° of knee flexion. Since reps were performed in a controlled cadence, we can calculate that subjects in the group training at long muscle lengths spent about 133 seconds per workout with their quads being “stretched” at a knee angle between 65-100° of knee flexion. So, if the effect was truly mediated by the “stretch” produced by training at longer muscle lengths, you’d expect:
- 12 weeks of “stretching” your quads once per week, for about two minutes, at a knee angle between 65-100° of knee flexion should cause about as much hypertrophy as doing 12 weeks of progressive resistance training though 30-65° of knee flexion.
- If subjects performed the same progressive resistance training though 30-65° of knee flexion and just added about two minutes of quad “stretching” once per week, at a knee angle between 65-100° of knee flexion, they would have achieved the same hypertrophy as the group performing progressive resistance training through 65-100° of knee flexion.
To be as clear as possible: “stretch” clearly isn’t mediating the effect observed in this study by Pedrosa et al. The reason I put “stretch” in quotes is that 100° of knee flexion is about 50° away from end-ROM knee flexion for most people (maximum knee flexion ROM tends to be around 150° in most individuals). So, if there was any stretch stimulus at all, it was an extremely low-intensity stimulus, performed for ~2-3% of the duration that is typically required for a (much higher-intensity) stretch stimulus to cause robust hypertrophy in humans.
Stretch-mediated hypertrophy can and does occur in humans. We do observe significant muscle growth when muscles are stretched at a high enough intensity and for a long enough duration. But the studies observing greater hypertrophy when training at longer muscle lengths do not present a sufficient stretch stimulus for the enhanced hypertrophy outcomes to be mediated by stretch. In other words, the increased growth response observed when training at longer muscle lengths isn’t, in the strictest sense of the term, “stretch-mediated hypertrophy.”
This may seem like a pedantic point, but it’s actually quite important for two reasons.
First, describing this phenomenon (increased muscle growth when training at longer muscle lengths) as “stretch-mediated hypertrophy” carries a misleading implication about the types of training that are required to take advantage of it. You don’t need to train near an end-ROM, or feel a deep stretch in the target muscle(s) in order to experience increased growth due to training at longer muscle lengths. However, if this phenomenon was described to you as “stretch-mediated hypertrophy,” you would naturally, and understandably, assume that you did need to train near an end-ROM, and you did need to feel a deep stretch in the target muscle(s) in order to take advantage of it. But, to this point, none of the studies observing increased muscle growth when training at longer muscle lengths actually involved training through maximal ranges of motion where a deep stretch would be achieved. It’s possible that training through the longest possible muscle lengths, and achieving a deep stretch on each rep would further enhance the effect (though there’s not yet human evidence to either confirm or refute that possibility), but it’s absolutely not necessary to achieve the effect.
Second, this is a budding area of research that still has a multitude of unanswered questions. However, if we describe this phenomenon as “stretch-mediated hypertrophy,” that presupposes that we already have all of the answers – the effect is mediated by stretch. In effect, describing this phenomenon as “stretch-mediated hypertrophy” entails jumping to a hasty (and very likely incorrect) conclusion about an intriguing topic that’s still poorly understood and ripe for continued exploration.
Why should we care about increases in fiber/fascicle length and pennation angle?
It’s important to explain why fascicle length and pennation angle increases are worth considering in this discussion. First, as already discussed, fascicle length increases appear to be one of the hallmark characteristics of the morphological adaptations to stretch training in animal studies. But, secondly – and more importantly – increases in fascicle length and pennation angle are a form of hypertrophy, at least the way we commonly measure hypertrophy. Not only do increases in fascicle length represent an increase in either the number of sarcomeres in series and/or the length of individual sarcomeres (all else being equal), but increases in fascicle length are also factored into measurements of cross-sectional area and muscle volume, as measured by MRI. Similarly, all else being equal, pennation angle increases also represent an increase in muscle size – increasing the radius in the cylinder example below (1). The same also applies to measurements of muscle thickness.
So, is the extreme stretch-mediated hypertrophy observed in animals entirely attributable to changes in fascicle/fiber length? Unlikely. While mean differences in fiber length changes observed are around +26.1 ± 7.3 % across the three studies that measured fiber length, the difference in hypertrophy observed in these same studies ranged from to +27.8% to +161.5%. Thus, while increases in fiber length certainly accounted for some of the change in muscle size observed, other adaptations, such as increases in fiber number and radial hypertrophy, also appeared to play a very important role. As a corollary, we can also assert that stretch-mediated hypertrophy is not just hypertrophy resulting from an increase in fiber length, but also an increase in fiber number (hyperplasia) and radial hypertrophy/pennation angle.
Similarly, in humans, things are rarely that straightforward, as changes in muscle size, pennation angle, and fascicle length have been known to occur in a relatively heterogeneous manner of ways in humans performing resistance training (1). For instance, though hypertrophy usually occurs alongside changes in fascicle length and pennation angle, there are studies in which muscle hypertrophy occurs in the absence of changes in fascicle length and pennation angle.
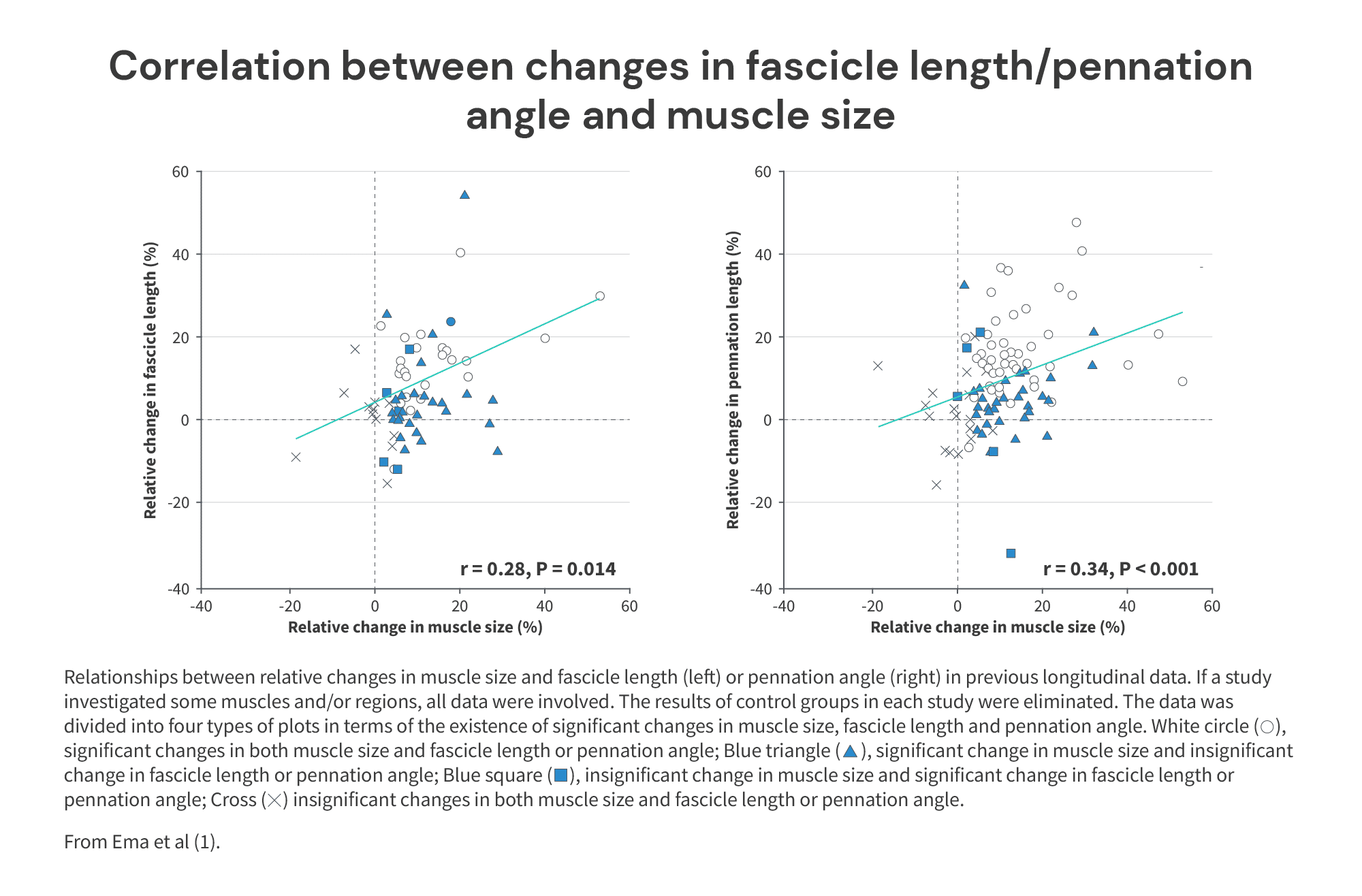
That said, when analyzing existing studies on fascicle length and muscle size changes from resistance training, a correlation of r = 0.28 was found, which is considered statistically “weak” or even “very weak.” Likewise, there was only a “weak” correlation of r = 0.34 between changes in pennation angle and changes in muscle size.
Therefore, in the ways we commonly measure muscle growth (i.e. increases in muscle volume/cross-sectional area through MRI and muscle thickness through ultrasound), increases in fascicle length at least have the potential to be responsible for differences in hypertrophy stemming from full ROM versus lengthened partials, but the observed association is relatively weak. However, even a weak association could be important if we consistently observe greater fascicle length adaptations from lengthened training, for example.
To be able to confidently assert that lengthened partials stimulate SMH (and not simply more hypertrophy), we need to examine whether lengthened resistance training stimulates greater increases in fascicle length and/or pennation angle compared to shortened resistance training. Additionally, if increases in fascicle length really are responsible for the benefit of lengthened partials, we should see that:
- Studies observing greater increases in fascicle length from lengthened training also generally find greater hypertrophy from lengthened versus shortened training.
- Studies not observing greater fascicle length increases from lengthened training also generally find similar hypertrophy from lengthened versus shortened training.
What forms of resistance training cause fascicle length adaptations?
Before we delve into the direct literature comparing fascicle length adaptations from more shortened versus more lengthened resistance training, it’s worth establishing how consistently – or not – resistance training stimulates increases in fascicle length. As it turns out, whether or not fascicle length even consistently increases in response to resistance training in humans remains slightly contentious within the scientific literature. Less than a decade ago, Fukutani and Kurihara (1) published a cross-sectional comparison of young male resistance trained lifters (bodybuilding and rugby athletes) to untrained lifters. In comparing the morphological characteristics of these two samples, they noted a few interesting findings. As you would expect, muscle thickness of the quadriceps (vastus lateralis) and calves (medial gastrocnemius) were substantially greater in the resistance trained lifters versus the untrained sample. Interestingly, though, fascicle lengths were similar between a relatively trained sample and a completely untrained sample, suggesting resistance training experience does not influence fascicle length. These findings prompted another group of researchers, Franchi et al (2016), to write a letter to the editor entitled “Fascicle length does increase in response to longitudinal resistance training and in a contraction-mode specific manner.” This is as close to “academic beef” as it gets.
In their letter to the editor, Franchi et al (1) argue that fascicle length adaptations to resistance training are more common than not; though there are some studies showing no fascicle length adaptations to resistance training, there is a greater number of studies that do show increases in fascicle length. Further into the argument, they highlight that the adaptations to resistance training are “somewhat” contraction mode-specific, such that concentric loading promotes increases in pennation angle (radial hypertrophy), whereas eccentric loading promotes increases in fascicle length (longitudinal hypertrophy).
To support this claim, a few studies comparing concentric and eccentric resistance training are cited. Performing a quick search of the data on eccentric versus concentric resistance training more broadly, we were able to find quite a few studies examining this topic. To briefly define concentric and eccentric muscle action:
- A concentric muscle action occurs when a muscle produces force and shortens (i.e. the way up during a squat).
- An eccentric muscle action occurs when a muscle produces force and lengthens (i.e. the way down during a squat).
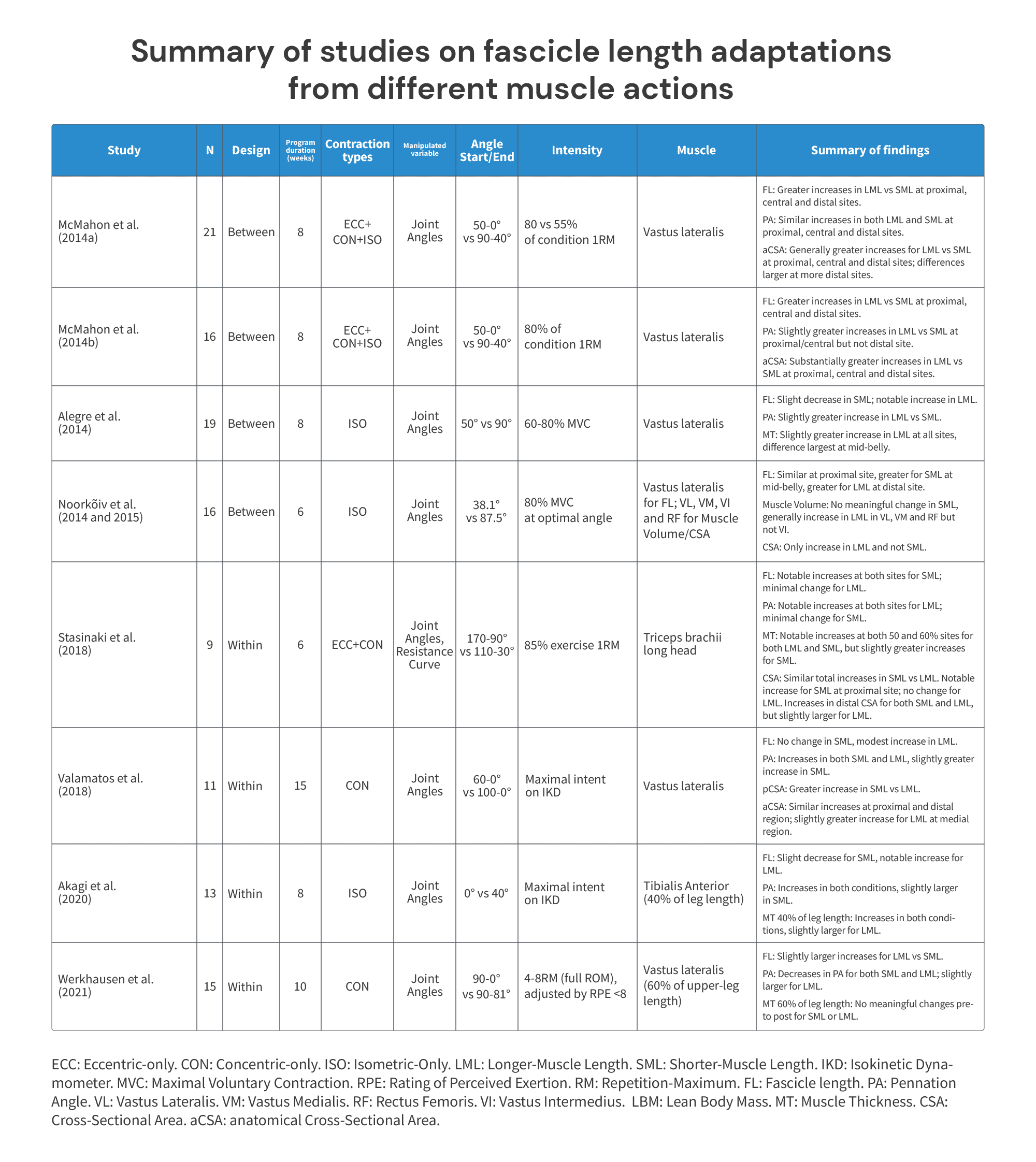
Below is a table summarizing the findings of the studies we were able to find comparing different modes of resistance training (e.g. concentric versus eccentric).
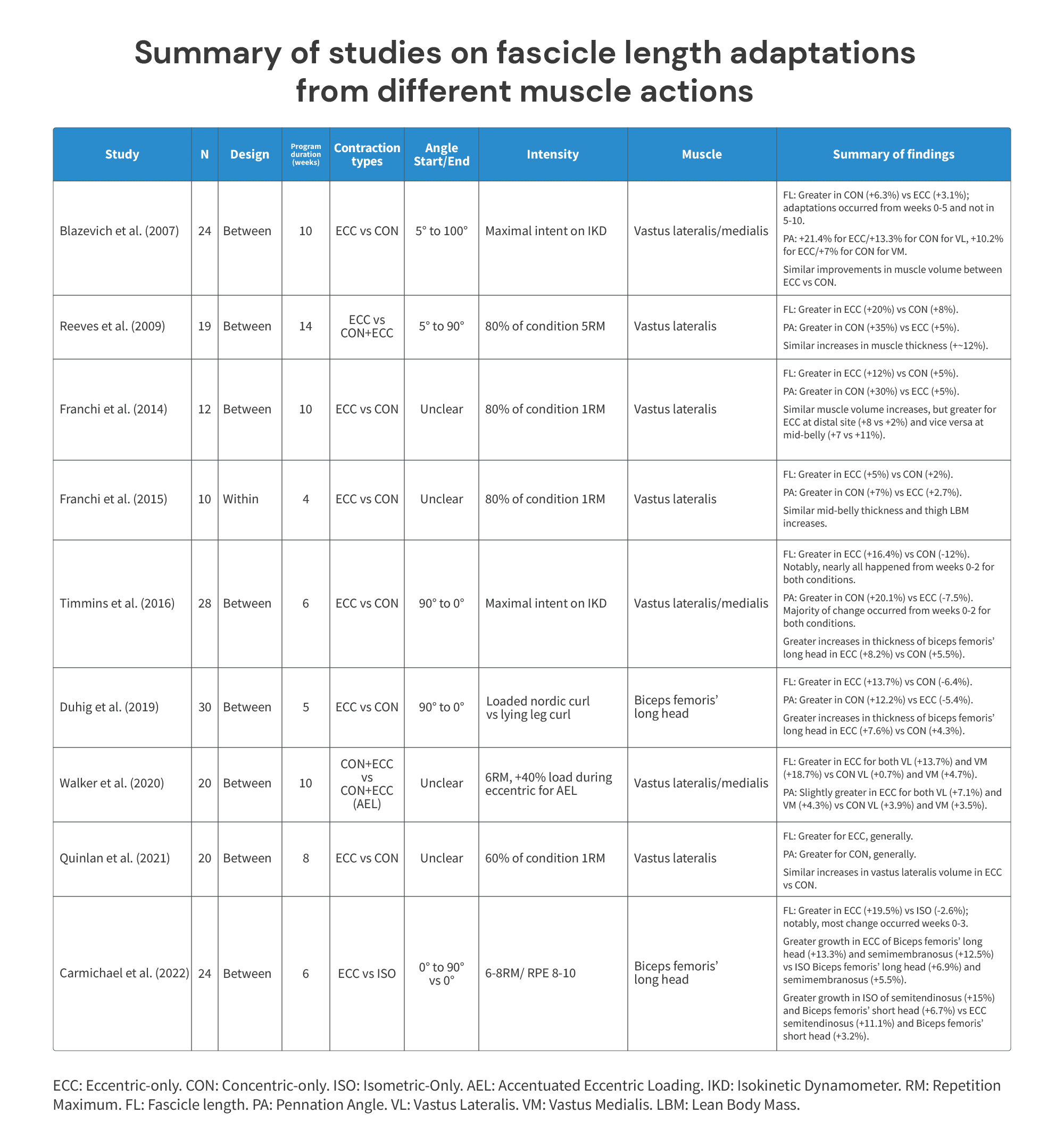
Notably, the study by Carmichael et al (1) included above also involved differences in muscle length trained, alongside comparing different muscle actions. In the eccentric condition, the knees were kept extended, but hips flexed from 0-90° of hip flexion. Conversely, in the isometric condition, both the hips and knees were kept fully extended (0° of hip flexion). As a result, since three of the hamstring muscles (biceps femoris’ long head, semimembranosus, and semitendinosus) are hip extensors, the eccentric condition trained at longer muscle lengths. Fascicle length increases were substantial in the eccentric condition (+19.5%), whereas the isometric training condition saw essentially no change (-2.6%). Likewise, hypertrophy results generally favored the eccentric condition for the biceps femoris’ long head/semimembranosus, but favored the isometric condition for the biceps femoris’ short head/semitendinosus.
Unfortunately, nearly all studies were conducted in participants who had no reported training experience. While this makes it difficult to determine whether these findings would generalize to more trained populations, there is one exception. The exception is the study by Walker et al (1), where participants had at least six months of training experience. Participants in both experimental groups (traditional and accentuated eccentric loading) performed concentric+eccentric training, with the only difference between groups being an additional 40% load added to the eccentric phase for the accentuated eccentric loading group. The accentuated eccentric group loading saw substantially greater increases in both pennation angle and fascicle length, suggesting these adaptations may take place even in more trained populations in response to a training approach accentuating the eccentric phase (such as an eccentric-only program).
Finally, these results are mirrored by a review paper by Franchi et al (1). Specifically, they found that not only did eccentric resistance training seem to increase fascicle length more than concentric resistance training, but it also led to larger increases in fiber cross-sectional area increases (Table 1.5 in the paper). This is important, since measurements of fiber cross-sectional area aren’t affected by increases in fascicle length. As a result, it’s extremely unlikely that the additional hypertrophy we’re observing is entirely attributable to superior increases in fascicle length from eccentric resistance training. So, while eccentric training seems to increase fiber length, it also just seems to cause more muscle hypertrophy overall.
Why do eccentric contractions stimulate greater adaptations in fascicle length?
Sharifnezhad and colleagues (1) compared the effects of (1) lower and higher load, (2) slower and faster velocity, and (3) shorter and longer muscle length eccentric-only contractions on fascicle length adaptations. Intensity was standardized between conditions by measuring maximum voluntary isometric contraction and using it to set torque on an isokinetic dynamometer. During a maximal voluntary isometric contraction (MVC), participants are essentially encouraged to push as hard as they can and exert as much force as they can against an immovable machine called an isokinetic dynamometer, which measures their torque/force output. The authors used this measurement to set intensity for training. Participants’ limbs were assigned to one of four conditions:
- Low load, 90 deg/s, 25-100 deg knee flexion.
- High load, 90 deg/s, 25-100 deg knee flexion.
- High load, 90 deg/s, 25-65 deg knee flexion.
- High load, 240 deg/s, 25-100 deg knee flexion.
Here are the adaptations in fascicle length between the different conditions (fascicle length was measured in different knee positions).
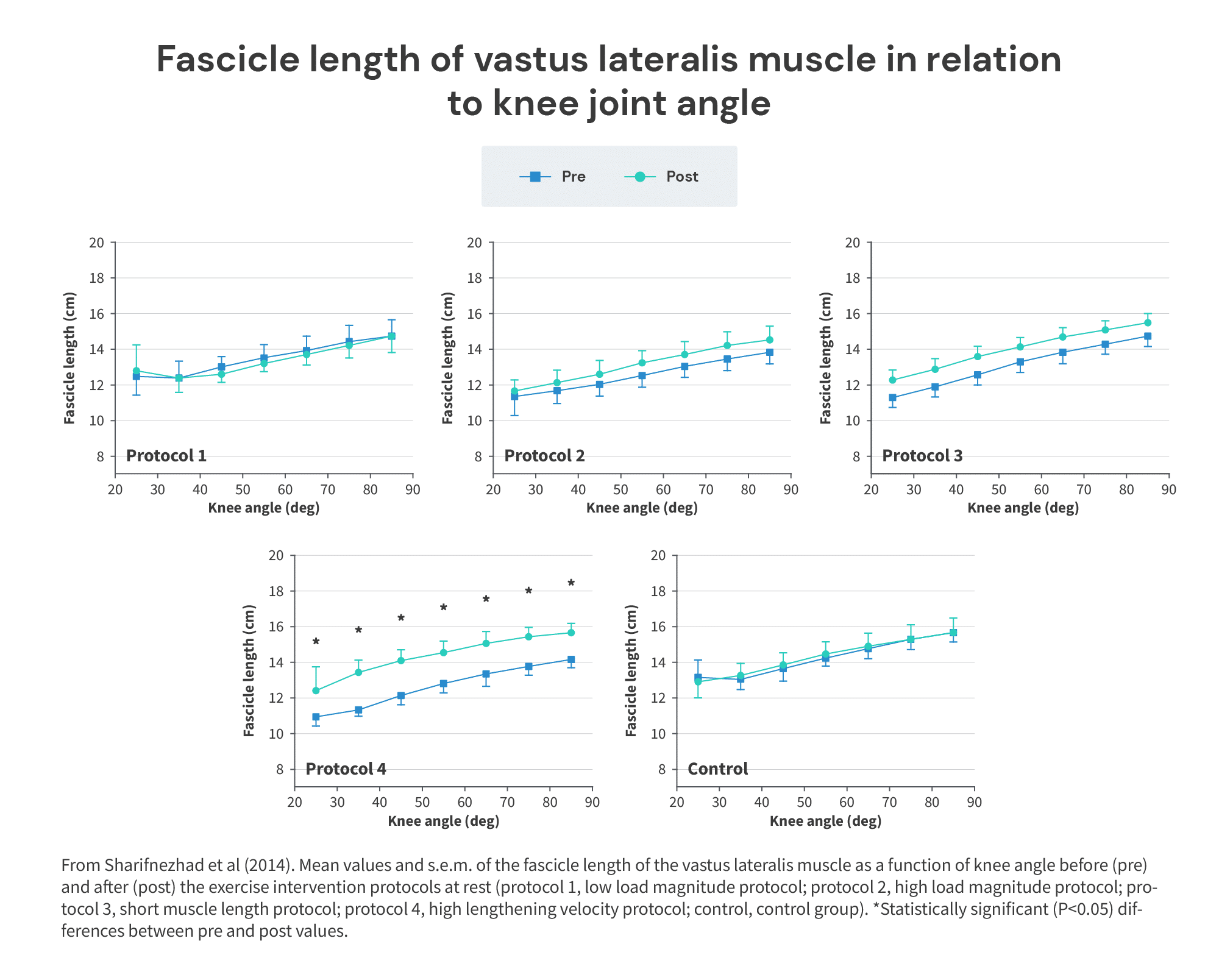
As you can see, fascicle length increases were generally greatest in the high-load, high-velocity condition, but both increasing load (condition 1 vs. 2) and increasing velocity (condition 2 vs. 4) appeared to potentially play a role. Additionally, muscle length did not seem to be a key determinant of fascicle length adaptations, since condition 2 (same load/velocity, longer muscle length) and condition 3 (same load/velocity, shorter muscle length) saw similar fascicle length adaptations.
Essentially, both increasing load/tension and lengthening velocity may play a role in increasing fascicle length adaptations. The former may be especially relevant here, in light of the takeaways from the research on concentric versus eccentric training from Table 5, as eccentric muscle actions allow you to generate more tension than concentric muscle actions (1). In light of the differences observed in the present study by going from 65% of MVC to 100% of MVC, some of the effect of eccentric contractions on fascicle length may have to do with this versus something inherently special about eccentric contractions. Additionally, muscle length itself may also not impact fascicle length adaptations much, at least during eccentric-only training.
Summary of concentric versus eccentric literature
To summarize the findings from Table 5, there are a few things we can conclude:
- Muscle growth from resistance training can occur alongside or in the absence of fascicle length/pennation angle increases.
- Eccentric-only training very consistently appears to increase fascicle length to a greater extent than concentric-only training.
- Even just accentuating the eccentric via added loading may increase fascicle length and pennation angle adaptations.
- The reason for this may simply be because we can produce more force during an eccentric versus concentric contraction.
- Concentric-only training consistently appears to increase pennation angle to a greater extent than eccentric-only training.
- Muscle hypertrophy changes generally appear comparable between eccentric-only and concentric-only training, but eccentric-only may have a slight edge (1).
- Higher load/intensity (e.g. %1RM) training may increase fascicle length adaptations.
- Faster velocity eccentric contractions may increase fascicle length adaptations.
So, we now know that resistance training can and does consistently increase fascicle length – at least in beginners and when performing the right type (i.e. eccentric contractions, predominantly).
However, based on the findings in the human stretching literature, it appears very unlikely that spending a few additional seconds at longer-muscle lengths per workout would be sufficient to meaningfully induce stretch-mediated hypertrophy.
Let’s review the data comparing shortened versus lengthened training.
Does lengthened training stimulate greater radial/longitudinal hypertrophy?
Takeaways
To summarize the table above, I think we can cautiously conclude the following:
- Training at longer-muscle lengths does generally increase fascicle length more than training at shorter-muscle lengths. This effect is notable.
- This suggests that lengthened partials may also result in notably greater longitudinal hypertrophy than shortened training.
- Training at longer-muscle lengths generally also increases pennation angle more than training at shorter-muscle lengths. This effect is modest.
- This suggests that lengthened partials may also result in slightly greater radial hypertrophy than shortened training.
- Fascicle length adaptations occur more quickly/dramatically in response to certain types of training (generally eccentric-only, at longer muscle lengths, with a faster tempo, and/or at a higher intensity/load).
- Much like muscle growth, fascicle length adaptations may occur quickly when you first begin training, but may slow down with experience.
To wrap this article up: I don’t think lengthened partials stimulate stretch-mediated hypertrophy – or, at least, not the way stretch-mediated hypertrophy was originally conceptualized. For one, human data suggests you’d need to spend way more time at longer-muscle lengths than you do when doing lengthened partials to stimulate a meaningful amount of stretch-mediated hypertrophy. There are still many gaps that would need to be addressed before we can confidently assert that stretch-mediated hypertrophy is at play when performing lengthened partials. Instead, it appears that more lengthened forms of training generally promote more muscle hypertrophy, across a wide variety of muscle actions, through a combination of notably greater increases in fascicle length/longitudinal hypertrophy and a slightly greater increase in pennation angle/radial hypertrophy.
The exact mechanisms underlying the additional hypertrophy observed from lengthened training/partials versus shortened training remain somewhat unclear. However, it is clear that we likely aren’t observing “stretch-mediated hypertrophy,” as it isn’t very likely that the effect is mediated stretch, as discussed above. If you’d like an in-depth discussion of other potential mechanisms, I would recommend checking out our previous article on range of motion.
If you made it this far, but were looking for practical applications, I would recommend both the article linked above and the practical recommendations made in our podcast episode on this topic.
FAQ
Does fascicle length only adapt in untrained lifters? Are lengthened partials only beneficial in beginners?
While lengthened training also appears to increase pennation angle to a lesser extent, the primary difference appears to be fascicle length mediated: lengthened training does consistently increase fascicle length to a greater extent than shortened training. Unfortunately, most of the studies on the topic were conducted in untrained participants. Therefore, an important question arises: Is this additional muscle growth short-lived and reserved only for beginners?
Several studies comparing different modes of resistance training and measuring fascicle length included measurements at a variety of timepoints (1, 2, 3). First, Blazevich et al (1) observed increases in fascicle length in both a concentric-only and eccentric-only group over 10 weeks. Interestingly, this adaptation plateau primarily took place during the first five weeks of training, with no further improvements from week 5 to week 10 of the intervention. Similarly, the aforementioned study by Timmins et al (1) had participants perform six weeks of either concentric-only or eccentric-only hamstring training and measured fascicle length at zero, two, three, and six weeks. Strikingly, in the eccentric-only group, fascicle length increased substantially from week zero to week two, then remained unchanged for the remainder of the six-week training intervention. Finally, a study by Carmichael et al (1) also examined changes in fascicle length from either eccentric-only or isometric-only training across six weeks, with measurements of fascicle length occuring in weeks zero, three, and six. In agreement with the two aforementioned studies, approximately two-thirds of the total increase in fascicle length took place between weeks 0-3; however, in slight contrast with the previous two studies, fascicle length continued to increase from weeks 3-6, albeit at a slower pace. These studies by Blazevich et al (1), Timmins et al (2), and Carmichael et al (3) seem to suggest that rapid fascicle length increases can occur within the first 2-3 weeks of performing training that tends to effectively induce increases in fascicle length (i.e. generally high angular velocities, eccentric-only training and very high/maximal intensities).
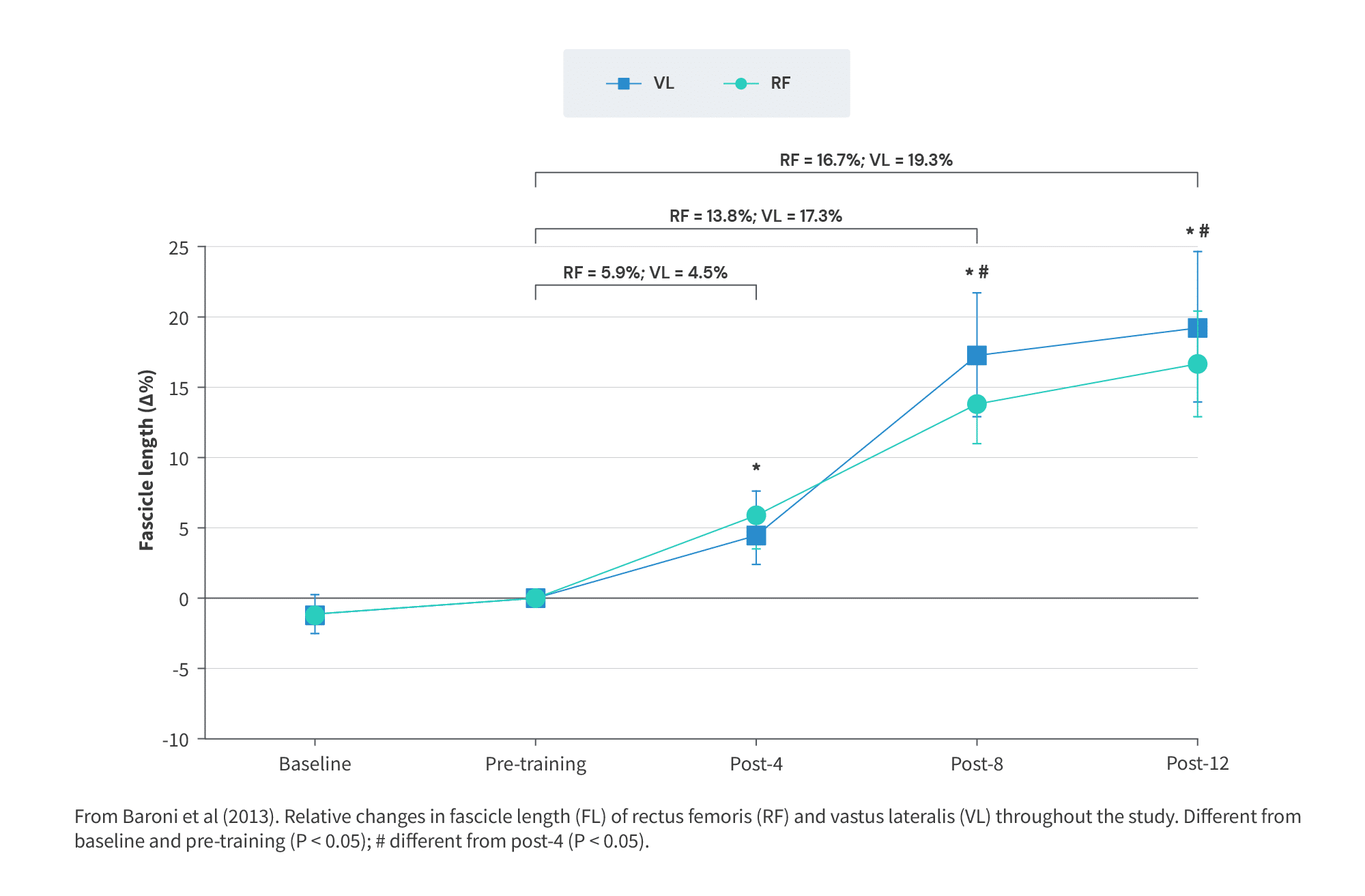
In contrast, a study by Baroni et al (2013) showed continuous and relatively linear increases in fascicle length during eccentric-only resistance training in the vastus lateralis and rectus femoris during the first eight weeks of the intervention. From weeks 8-12, increases in fascicle length appeared to slow down, but didn’t cease altogether. This study suggests that fascicle length adaptations may not plateau after only 2-3 weeks.
Likewise, a study by Anousaki et al (1) in male throwing athletes broadly supports the idea that fascicle length adaptations can occur in trained lifters. In the lead-up to the national championships, this study followed these elite athletes through a 25-week macrocycle, consisting of three training blocks performed in the following order:
- 12-week hypertrophy and strength phase.
- 9-week maximum strength and power phase.
- 3-week power and speed phase.
Measurements of performance and muscle architecture (including fascicle length) were taken before the start of the 25-week block, between each phase, and at the end of the 25-week macrocycle. While this population probably didn’t place a ton of focus on eccentric-only training or the lengthened position in their usual training, they were certainly a well-trained population, with an average squat 1RM of ~180kg or ~405lbs. During phase one, there was very little adaptation in fascicle length (+~1.1% over 12 weeks). However, phase two and phase three appeared to meaningfully increase fascicle length (+8.5% over 12 weeks). While the small sample size and lack of randomization make it difficult to draw a clear causal relationship, the primary difference between phase one and phase two appears to be an increase in the training intensity/%1RM, which could potentially contribute to greater adaptations in fascicle length. Unfortunately, details regarding the exact exercise selection were omitted, which makes it difficult to even surmise whether an increased emphasis on the stretched position could be at play. In line with these results, a similar study by the same group of researchers also found meaningful increases in fascicle length (+13.4%) during the five-week strength/power phase of a resistance training macrocycle in well-trained throwing athletes with a squat 1RM of ~125kg/275lbs (in a mixed sample of males and females).
At the very least, these three studies collectively suggest that increases in fascicle length can still occur, even in well-trained lifters. Overall, the evidence suggests that though fascicle length adaptations may decrease as training status increases, adaptations can occur even in trained lifters. It’s also plausible that, for well-trained lifters who haven’t focused on the lengthened position/used lengthened partials yet, this could result in additional muscle growth.
Importantly, we need to be cautious in making extrapolations about the long-term impact of lengthened partials on muscle hypertrophy on the basis of this short-term research. For one, fascicle length does appear to increase, albeit to a lesser extent, even in trained lifters, suggesting that there is still a benefit to lengthened training, assuming it is the mechanism behind the additional hypertrophy seen from lengthened training. Additionally, we have evidence that lengthened training – across a variety of muscle action types – leads to greater increases in muscle growth, fascicle length, and (to a lesser extent) pennation angle. There may also be a dose-response relationship, wherein increasing the muscle length during training amplifies these differences. In the studies comparing longer muscle length RT to shorter muscle length RT, the muscle length during the longer muscle length training is rarely maximized. Considering that you may be training at longer muscle lengths in the real world versus what is tested in these studies, you may see different/greater adaptations in muscle growth, fascicle length, and pennation angle. All in all, many questions remain.
Are our measurements of fascicle length even accurate?
An important limitation of most the studies conducted on fascicle length has to do with the validity and reliability of measuring fascicle length in vivo. The exact methods used to measure vary somewhat between studies, but one common issue is that the width/field-of-view of many ultrasound transducers is too small to visualize the fascicle fully in a single image. To circumvent this issue, some studies use manual linear extrapolation, wherein a formula is used to estimate the full length of the fascicle on the basis of visualizing only a segment of the full fascicle during regular field-of-view ultrasonography. Alternatively, a few different trigonometric equations based on muscle thickness, angle between aponeuroses, pennation angle, and the visualized segment are also sometimes used. These methods essentially assume that the fascicle is a straight line, allowing us to estimate its full length based on visualizing only a segment. Unfortunately, this is problematic: in hypertrophied muscle, fascicles can often become curved/non-linear, rendering the result of linear extrapolation less accurate (1).
The most accurate method of measuring fascicle length in vivo (in live humans) is by using an extended-field-of-view ultrasound device, which allows us to visualize and measure the whole fascicle without relying on extrapolation methods. However, extended-field-of-view ultrasound devices are rare and expensive. As a result, most studies on fascicle length from concentric versus eccentric training and shortened versus eccentric training rely on one of the extrapolation methods detailed above.
Generally, the manual linear extrapolation method has excellent agreement with the extended-field-of-view method; their results appear very comparable (r = 0.83). In contrast, relying on trigonometric extrapolation methods was generally much less accurate, with these methods showing relevant biases compared to extended-field-of-view ultrasound (1).
There are a few things to take away from this study. First, since fascicle length measurement isn’t perfectly accurate (especially when relying on extrapolation methods), it becomes even more important to rely on multiple studies to inform our practices. Second, since most studies do not use extended-field-of-view ultrasonography, this may partly explain why the correlation between fascicle length increases and hypertrophy is relatively weak (r = 0.29) and why some studies can observe changes in muscle size without changes in fascicle length and pennation angle (1).
Fascicle length increases: sarcomerogenesis or increase in sarcomere length?
Throughout the article, you’ll notice I do not refer to fascicle length increases as an increase in serial sarcomere number (or sarcomerogenesis). There are a few reasons for this.
First, it’s important to understand that an increase in fiber or fascicle length can be caused by a two distinct adaptations: either by an increase in the number of sarcomeres that make up the length of the fascicle, and/or by an increase in the length of the individual sarcomeres that make up the length of the fascicle. Importantly, sarcomere length is also known to be heterogeneous, meaning sarcomeres in the same fiber/fascicle can vary in length. While increases in serial sarcomere number are reasonably consistent and well-documented in animals and are commonly responsible for increases in fiber length, this same relationship is not yet established in humans.
The main reason I referred to adaptations in fascicle length (and not serial sarcomere number) is that none of the studies in humans performing stretching interventions or resistance training (concentric versus eccentric, shortened versus lengthened) actually measured serial sarcomere number. Instead, they measured fascicle length. There’s a simple reason for this: measuring serial sarcomere number is much easier when you can sacrifice the participant (as is the case in animal models) and dissect them. In vivo/in live humans, measuring serial sarcomere number is much trickier.
While there have been advances in technology over the past few years enabling us to measure serial sarcomere number in humans, using a combination of ultrasonography and microendoscopy, the equipment required is still relatively rare and virtually no studies have actually measured changes in serial sarcomere number in humans performing resistance training. There is one exception, though, and that is a recent study by Pincheira et al (1), which is the only study to have estimated serial sarcomere number and sarcomere length changes in response to resistance training in humans.
Ten recreationally active participants did Nordic curls for three weeks. As we reviewed throughout the article, Nordic curls are a great candidate for increasing fascicle length on account of (1) being eccentric-only and (2) exposing the hamstrings to longer muscle lengths. Fascicle length, serial sarcomere number, and sarcomere length were measured at the mid-belly and distal portion of the biceps femoris’ long head, before and after the three-week training phase. No changes in fascicle length, sarcomere length, or sarcomere number were observed at the mid-belly site. However, at the distal site, increases in fascicle length from pre- to post-training were observed. Specifically, the authors observed a 21% increase in fascicle length alongside a 17% increase in sarcomere length, explaining nearly all of the adaptation in fascicle length. In contrast, the number of sarcomeres remained unchanged. These findings suggest that, in humans, increases in sarcomere length may be responsible for increases in fascicle length rather than increases in serial sarcomere number.
To summarize: In humans, we don’t fully understand what structural adaptations underlie increases in fascicle length yet. Increases in fascicle length are a type of muscle hypertrophy, but whether they occur as a result of increases in serial sarcomere number or increases in sarcomere length remains to be determined.


