

Note: This article was the MASS Research Review cover story for January 2023 and is a review of a recent paper by Albarello et al. If you want more content like this, subscribe to MASS.
Key Points
- The present study (1) measured acute EMG and muscle swelling (thickness and cross-sectional area, assessed via ultrasound) responses in the upper and mid chest after flat and incline benching.
- A previous study (2) reported greater longitudinal upper chest hypertrophy and similar mid chest hypertrophy when comparing incline to flat benching.
- EMG responses differed in a predictable manner in the present study, with incline bench causing higher upper chest activity and flat bench causing higher mid chest activity. However, muscle swelling outcomes differed from the EMG outcomes, and also failed to comport with the longitudinal hypertrophy data from the prior study.
Regional hypertrophy is the well-established phenomena (demonstrated here, here, and here) where non-uniform growth occurs in a muscle or muscle group. For example, if your biceps grew more near the elbow in response to training than they did near the shoulder, that would be an example of regional hypertrophy. In another example, Greg previously reviewed a study by Chavez and colleagues in which a group of untrained males performing incline bench press only, flat bench press only, or a mixture of both, experienced different hypertrophy patterns in the upper and mid pecs (2). Interestingly, there were no significant differences between groups, except that the incline bench press only group had a significantly greater (and quite substantial) increase in their upper chest thickness (i.e., the clavicular head of the pectoralis major) compared to the other two groups. To my knowledge, this is the only study examining longitudinal regional pec hypertrophy differences between groups performing different pressing exercises; however, there are a fair number of studies looking at acute responses (such as EMG) that you might think would provide some indication of what regional hypertrophy responses you’d get long term (3, 4). The present study (1) in an interesting example, as the participants performed flat and incline bench press sessions while the researchers examined their upper chest and mid chest (i.e., the sternal head of the pectoralis major) EMG activity, and ultrasound-derived muscle swelling (i.e., acute muscle thickness and cross-sectional area changes) following training. This design allows us to compare these two acute proxy measures to see how they comport with one another, but we can also see if either acute measure lines up with the one existing study on longitudinal hypertrophy following incline and flat bench pressing (2). As one might expect, EMG activity was greater for the upper than the mid chest during incline bench press and the opposite was observed during flat bench, and these differences were significant between exercises. However, as I’ll discuss in this article, the normalization procedures used in the present study make it difficult to conclude much from these findings. Muscle swelling increased to a greater extent in the upper than the mid chest following the incline bench, and the opposite pattern was observed following the flat bench. However, when comparing absolute muscle swelling between exercises, the only significant difference was that mid chest swelling was greater following flat bench than incline bench, but notably, upper chest swelling was similar after both bench press variations. Therefore, acute muscle swelling did not follow the pattern of longitudinal regional hypertrophy observed in the one existing training study (2). In this review I’ll discuss the detailed findings of the current study and how they inform our ability (or lack thereof) to predict regional hypertrophy in response to specific exercise variations.
Purpose and Hypotheses
Purpose
The purpose of this study was to determine if there are differences in surface EMG during, and muscle thickness and cross-sectional area after the incline and flat bench press in specific regions of the pectoralis major. Further, this study aimed to clarify whether “the muscle region of the pectoralis major with the highest sEMG [surface EMG] amplitude during exercise corresponds to the one with the greatest acute variations in cross-sectional area and/or muscle thickness.”
Hypothesis
The authors hypothesized “that the pectoralis major head with the greatest sEMG amplitude during exercise will be the one with the greatest acute variations in muscle architecture [i.e., muscle thickness and cross-sectional area].”
Subjects and Methods
Subjects
Thirteen injury-free, resistance-trained males (28.79 ± 4.46 years old; 174.64 ± 5.60cm tall; weighing 79.43 ± 8.99kg) participated in this study. Participants needed to have at least one year of resistance training experience, not be regularly performing other forms of physical activity, and have a 1RM flat bench of at least their bodyweight.
Study Design
The participants attended four lab sessions. The first two were 1RM sessions and the last two were experimental training sessions. Specifically, the first session was a familiarization which included ultrasound measurements and a 1RM assessment where the participants tested both the flat and 45° degree incline bench press with 30 minutes rest between the two. The second session was a repeat of the first session that was performed for reliability purposes. I believe the exercise order of the 1RM test days was randomized, as exercise order was randomized in the training sessions, but this was not explicitly clear. The third session occurred 72 hours after the second 1RM testing session, and consisted of four sets of the flat or incline bench press (the exercise that was performed on each day was randomly determined) to failure with 60% of 1RM, during which pec EMG activity was recorded, and after which muscle swelling was captured. The fourth and final experimental session occurred 96 hours after the third session (the additional day was provided to allow for muscle damage recovery), and was a repeat of session three with the bench variation that had not yet been performed. The participants rested at least three minutes between these four sets on both days. Participants were asked to avoid any strenuous activity during the study.
EMG
Electrodes were placed on the clavicular and sternal head of the pectoralis major as shown here. EMG data were reported as the root mean square (RMS) of activity during the concentric phase of each rep within each set. Essentially, the RMS tells you the average power of the electrical signal from the muscle over the time period sampled. These RMS values for each head of the pec were normalized within each exercise separately to the highest RMS value observed for the specific pectoral head during each set. Meaning, the average EMG values for each pec region were scaled to their own peak within each exercise. Unfortunately, this presents a substantial limitation which prevents meaningful comparisons between muscle regions within, and between exercises. If you’re interested, the specifics of what the EMG findings in this study can tell you I discuss in the Criticisms and Statistical Musings section.
Ultrasound-Derived Muscle Swelling
Changes in muscle thickness and cross-sectional area (which I refer to collectively as changes in “muscle swelling” in this article) were derived from panoramic ultrasound images guided by a custom made support to increase probe stability and standardize probe placement as shown here. The percentage change in cross-sectional area and muscle thickness was calculated by comparing the average thickness and cross-sectional area values from before to after each training session. The same technician analyzed all the images.
Findings
Reliability
The authors ensured an accurate relative load selection by recruiting trained participants with experience in the bench press, by having a familiarization session, and by repeating their 1RM tests twice to ensure reliability. Likewise, they took ultrasound measurements on each 1RM testing day to ensure muscle thickness and cross-sectional area reliability. They reported their reliability statistics, which aren’t worth discussing in detail in this review. But, in summary, reliability was quite good, indicating that we can have confidence in the reported values.
EMG
As shown in Figure 1, within each exercise there was a significant difference reported in sternal and clavicular head EMG activity. The authors reported that flat bench press produced more activity (~30 %; p < 0.001) in the sternal than the clavicular head in every set, while the incline bench press produced more activity (~34%; p < 0.001) in the clavicular than the sternal head in every set. While these findings are intuitive, due to the normalization procedures, we actually can’t make inferences about relative excitation between the pectoral regions.
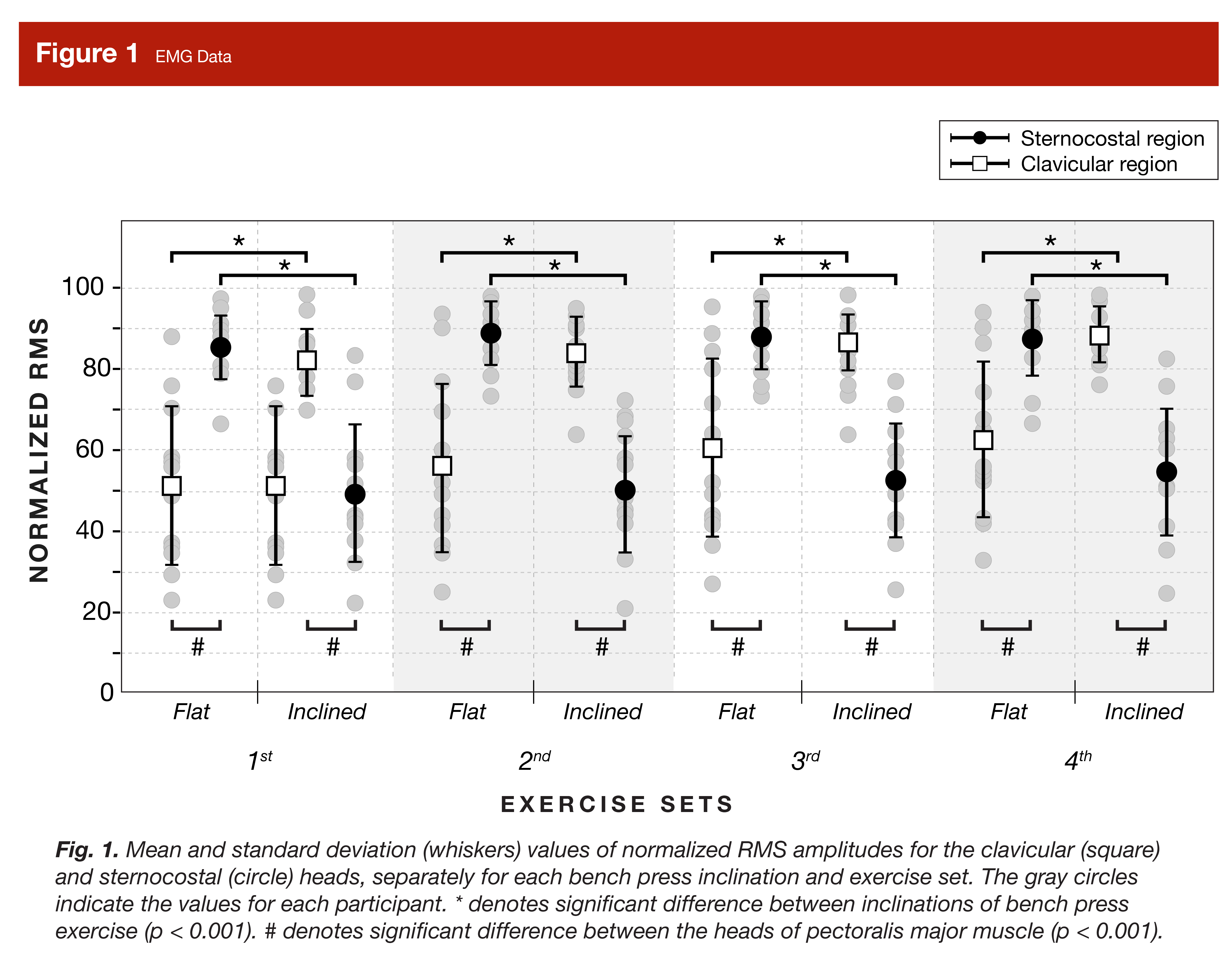
Likewise, the authors reported that the flat bench produced significantly more sternal activity than the incline bench press (~35%, p < 0.001), while the incline bench press produced significantly more clavicular activity than the flat bench press (~28%; p < 0.001). However, once again, these between-exercise muscle activity comparisons should also be interpreted with caution, if made at all (see the Criticisms section).
Muscle Swelling
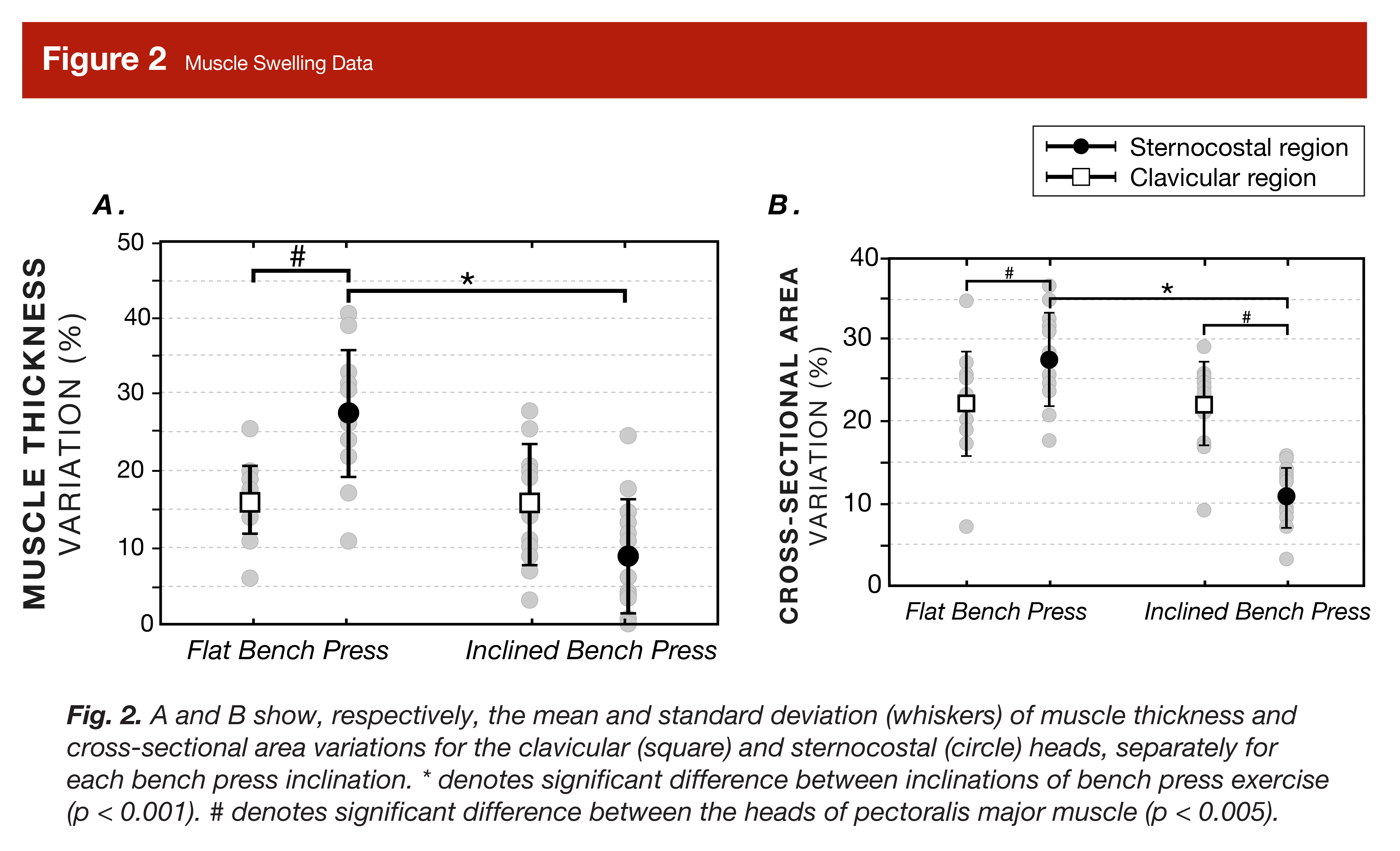
As shown in Figure 2, muscle swelling responses differed between pectoral regions within-exercise, and between exercises. After flat benching, the participants’ sternal head increased in thickness significantly more than their clavicular head (~11.06%; p < 0.005) and this pattern held true for cross-sectional area (~5.42%; p < 0.005). Conversely, after incline benching, the participants’ clavicular head cross-sectional area increased significantly more than their sternal head (~10.81%; p < 0.001), and although this pattern roughly held true for muscle thickness, it was not significant (~6.83%; p = 0.08). Notably, however, the only between-exercise differences in muscle swelling were that the flat bench press produced significantly greater increases in muscle thickness (~3-fold; p < 0.001) and cross-sectional area (~17.89%; p < 0.001) in the sternal head compared to the incline bench press. Further, the increases in clavicular pec muscle swelling were not significantly different between incline and flat bench (p = 0.842-0.992), and in fact, appeared quite similar visually.
Criticisms and Statistical Musings
As I’ve mentioned earlier in this article, the EMG data from this study don’t allow many useful inferences to be made. Initially when I wrote this article, I thought only the between-exercise data was subject to this limitation, but Greg thankfully (but unfortunately) caught that it also applied to the within-exercise data. To understand this limitation, we need to discuss normalization. Normalization is the process by which you scale raw EMG data into more usable information. But, which raw EMG data you choose to be scaled and what you scale it to, is very important. Notably, in this study, the authors used the average EMG activity for each pec region during each set for each exercise, and normalized it to the highest EMG activity produced by that same pec region, within that same set. This gives you the ratio of the average EMG activity of each pec region to its own peak EMG, during each set of each exercise. So, if a pec region reached a peak that actually was equal to its theoretical max excitability (which we wouldn’t know), and stayed at 90% of that peak value on average during each set, its value would be 90% (out of 100%). However, if the pec region reached a peak that actually was equal to only half of its theoretical max excitability (which again, we wouldn’t know), and stayed at 90% of that peak value on average, its value would also be 90%. Meaning, all these values really tell us are how close to the highest EMG activity (which may or may not have been very high relative to the muscle’s maximum capacity) recorded in each set was the average EMG activity in each set. If you’re wondering “ok, so what does that tell me?” Unfortunately, the answer is not very much. If you wanted to know the relative differences in muscle-specific EMG activity within and between the two lifts, EMG activity would need to be normalized to a theoretical muscle-specific maximum value, like a maximum voluntary isometric contraction (MVIC). An MVIC is exactly what it sounds like, an isometric contraction done with maximum effort using a joint angle that should provide a muscle-specific theoretical maximal EMG excitation value which can then be used as a reference across exercises (as I discussed here in more detail in the “limitations of EMG” section). Since the authors didn’t use this approach, you can’t actually make any inferences about relative EMG activity between pec regions, within or between exercises. With all that said, it’s worth mentioning that normalizing data to an MVIC introduces other limitations. There are assumptions as to whether MVIC performances represent true maximums, which also extend to the exercises they are compared against. Joint angle differences between exercises acutely alter muscle morphology and position, subsequently impacting EMG signal strength and acquisition. In addition, not all muscles have the same recruitment pattern. Some follow a superficial to deep pattern, while others deep to superficial, which can understandably impact surface EMG (5). Therefore, comparisons between different exercises which train the same muscle, even when based on MVICs, may not be valid representations of relative signal strengths, and therefore of expected longitudinal hypertrophy differences (6).
I have one final note, unrelated to EMG, which is a defense against potential criticisms rather than a criticism of this article. Some could reasonably disagree with how I’ve positioned differential hypertrophy in the upper and mid chest due to exercise selection as “regional hypertrophy.” While the clavicular and sternal heads of the pecs are both part of the pectoralis major, and not considered separate muscles, they are innervated by different motor nerves (7). Thus, they arguably function more like separate muscles than regions of the same muscle. In a prior era, say a decade ago, when the “evidence-based” community was generally skeptical of the concept of regional hypertrophy, you might hear someone point this out and claim a differential hypertrophy response in the upper versus mid chest was therefore not evidence of regional hypertrophy. However, at this point, with more awareness of the many studies showing the occurrence of regional hypertrophy, I didn’t think it was a distinction worth quibbling over. For completeness I wanted to acknowledge this nuanced point, but from a bodybuilding perspective, it’s immaterial, as it’s simply useful to know what exercises might be more effective for growing the upper and mid chest.
Interpretation
It would be nice to be able to predict which exercises reliably produce specific regional hypertrophy in specific muscles. As a competitive bodybuilder and a coach of physique athletes, I want that to be our reality. Unfortunately, we just aren’t there yet. Moreso, we need more data to determine which acute proxy measures might be able to predict hypertrophy long term, but we also have to accept that there will always be inherent limitations to such predictions.
To start, let’s summarize where we are with predicting regional hypertrophy based upon exercise selection. As I mentioned in the Methods and Criticisms sections, the EMG data in this study unfortunately can’t tell us very much. Despite this, it is still an important reminder regarding the challenges and complexities of predicting long term adaptations from acute measurements which each have their own unique limitations. Notably, while EMG activity is useful in other ways, it is limited in its ability to compare the hypertrophy stimuli between exercises (5, 6). On the other hand, I can’t think of any reason why you can’t make valid muscle swelling comparisons between exercises. Interestingly, the muscle swelling findings suggest that flat bench press is an all around better exercise than incline for both upper and mid chest development (if we assume muscle swelling is indicative of the stimulus). Specifically, the flat bench produced greater increases in the thickness and cross-sectional area of the mid chest compared to incline, and similar increases in the upper chest. But what does acute muscle swelling really tell us? Well, a rationale to use it as a proxy measure for hypertrophy might be that increases in swelling could indicate increased blood flow, edema, and metabolic activity (which might be experienced as a greater pump) in a given region, likely due to work being performed by those specific muscle fibers. Indeed, there are some (albeit not strong) relationships between acute changes in muscle size and longitudinal hypertrophy (8).
So, if we take the muscle swelling results at face value, we’d conclude that flat bench press is an overall superior chest builder compared to incline, as it better stimulates the mid chest and provides a similar stimulus to the upper chest. Further, we’d conclude that the anecdotal experiences of lifters that incline is a better upper chest developer are therefore incorrect. This could be true. Anecdotal experiences can be confounded by a lot of factors, and furthermore, individual differences can be amplified by loud or prominent voices and unduly influence what becomes “collective wisdom.” For example, imagine that a prominent bodybuilder with a strong influence in the community did actually get more upper pec hypertrophy from incline compared to flat bench due to their individual biomechanics, and then reported their experience as if it was the norm, when in fact, most people wouldn’t respond the same way. This type of thing happens, however, we don’t have to make this shaky, speculative comparison between a proxy measure and anecdotal evidence. Rather, we can make a slightly less shaky and speculative comparison (but just slightly) between the present study with existing data on hypertrophy.
As I mentioned in the introduction, Greg previously reviewed the only study I’m aware of in which the authors compared longitudinal changes in regional hypertrophy between groups performing only flat bench, incline bench, or a combination of the two (2). Unfortunately, their findings were directly contrary to what you’d expect based on the muscle swelling data in the present study, as the incline only group experienced significantly greater upper pec hypertrophy than both of the other two groups, with no other differences between groups. Therefore, while the present acute data indicates the flat bench is a hands-down better exercise for pec development in all regions compared to incline, the actual research on hypertrophy suggests the opposite. If your reaction to this comparison is that we should place more faith in the actual longitudinal hypertrophy findings, in principle, I agree with you. However, it’s worth noting that we only have this one study by Chavez (2) to go on, and, as Greg noted in his interpretation, the findings are a little odd. Specifically, upper pec thickness increased by more than 62% in the incline pressing group, which is an unheard of increase that stands out as an outlier compared to other studies. The reason for this massive degree of hypertrophy reported by Chavez is unknown, but to be clear, neither I nor Greg are calling foul. As discussed in Greg’s article, besides the magnitude of change, the data don’t look “funky.” So this finding could be accurate, but just confounded by other factors which inflate its magnitude such as muscle swelling (the measurement was taken within 24-48 hours of the last training session), the use of untrained subjects, poor measurement reliability, a combination of these factors or perhaps other, unknown variables. Nonetheless, we need more research to clearly determine the effects of incline and flat bench press on regional pec hypertrophy.
To give you my personal take, it doesn’t make sense to me that flat bench press is just as effective at inducing upper chest hypertrophy as incline bench and it also doesn’t make sense that incline bench is just as good as flat bench at inducing mid chest hypertrophy, and of course, the two are mutually exclusive conclusions. This means I have to question both the findings of Chavez and the relevance of the muscle swelling findings in the present study. This puts me in a difficult spot, as I actually think it’s reasonable to speculate that differences in acute muscle swelling might be grossly predictive of long term hypertrophy. However, I think there might be a plausible explanation for why muscle swelling favored flat bench press. If you look at the inclusion criteria, the participants had a strength requirement for flat bench, but not incline. Thus, it’s possible that the trained participants were more trained on flat bench press than incline, and just couldn’t induce as much of a stimulus with the less familiar movement. While this sounds plausible, it’s admittedly not a rock solid explanation. If you look at the reliability data for the 1RM tests, both exercises were similarly reliable, and the participants’ incline bench 1RM was ~85% of their flat bench press 1RM, which seems like a reasonable percentage. Another possibility that Greg brought up, is that it could be related to posture. Since you’re sitting more upright with incline, that could just promote better venous drainage/less blood pooling during exercise, resulting in less swelling at the time of measurement. While possible, ultimately, I don’t have a good explanation for the (in my opinion) non-intuitive between-exercise muscle swelling differences, but it might just be that acute muscle swelling (and by proxy, your acute perception of a pump) just aren’t that useful as proxies for the hypertrophy stimulus.
On that note, I think we simply need to test more proxy measurements such as T2 MRI (as discussed here), and perhaps muscle oxygenation (as discussed here) in addition to EMG activity (normalized differently) and muscle swelling, as well as more practical measurements like “perceived pump” and subjective assessments of muscle soreness after training to see if and how they associate with longitudinal changes in regional hypertrophy. However, even if we conduct such experiments, we have to set realistic (i.e., low) expectations for these proxies’ predictive abilities. To illustrate why, imagine an experienced lifter who needs a given amount of volume and effort to maintain their muscle size. Then, imagine that the lifter reduced their training to 1/10th of that volume for an extended period of time while maintaining high effort. Likely, they would slowly start getting smaller; however, if you took a battery of measurements during and after one of their effortful, reduced-volume sessions, you’d see plenty of EMG activity in the trained muscles, increased T2 MRI and muscle oxygenation in those same muscles, the lifter would get a pump and get sore afterwards (probably more than normal due to a degradation of the repeated bout effect), and they’d also experience large increases in acute muscle swelling. However, they’d still be getting smaller. My point is, there is a lot that goes into the outcome of hypertrophy, and no matter how good a proxy is, it simply can’t capture all the variables which influence it.
To conclude, the present study is really interesting. It demonstrates unique EMG activity in the upper and mid chest during flat and incline bench pressing and distinct regional-specific muscle swelling responses. While these responses don’t comport with the current incline and flat bench longitudinal hypertrophy data we have, this area is ripe for further research.
Next Steps
As I alluded to in the interpretation, there are two avenues for future research I’m interested in. For one, we need additional longitudinal research on hypertrophy following incline compared to flat bench press training to see if the observations of Chavez and colleagues (2) can be replicated. Additionally, we need longitudinal hypertrophy research that follows baseline proxy measures that might predict hypertrophy like T2 MRI, muscle oxygenation, and practical measures of subjective soreness and pump quality to see what relationships are strongest, and if they are regionally accurate. With this research conducted we might be able to potentially make better inferences about long term adaptation based on acute studies and possibly use certain proxies for training monitoring purposes as well.
Application and Takeaways
- We don’t yet have good acute proxy measures to accurately predict hypertrophy broadly, let alone in a region specific manner. The present study demonstrates differences in muscle activity during flat and incline bench training, and muscle swelling following flat and incline bench training in the upper and mid chest. While intriguing, we need further research to determine if these data are reasonable proxies for predicting long term adaptation.
Get more articles like this
This article was the cover story for the January 2023 issue of MASS Research Review. If you’d like to read the full, 126-page January issue (and dive into the MASS archives), you can subscribe to MASS here.
Subscribers get a new edition of MASS each month. Each edition is available on our member website as well as in a beautiful, magazine-style PDF and contains at least 5 full-length articles (like this one), 2 videos, and 8 Research Brief articles.
Subscribing is also a great way to support the work we do here on Stronger By Science.
References
- Albarello JCDS, Cabral HV, Leitão BFM, Halmenschlager GH, Lulic-Kuryllo T, Matta TTD. Non-uniform excitation of pectoralis major induced by changes in bench press inclination leads to uneven variations in the cross-sectional area measured by panoramic ultrasonography. J Electromyogr Kinesiol. 2022 Dec;67:102722.
- Chaves SFN, Rocha-Júnior VA, Encarnação IGA, Martins-Costa HC, Freitas EDS, Coelho DB, et al. Effects of Horizontal and Incline Bench Press on Neuromuscular Adaptations in Untrained Young Men. Int J Exerc Sci. 2020 Aug 1;13(6):859-872.
- Rodríguez-Ridao D, Antequera-Vique JA, Martín-Fuentes I, Muyor JM. Effect of Five Bench Inclinations on the Electromyographic Activity of the Pectoralis Major, Anterior Deltoid, and Triceps Brachii during the Bench Press Exercise. Int J Environ Res Public Health. 2020 Oct 8;17(19):7339.
- Trebs AA, Brandenburg JP, Pitney WA. An electromyography analysis of 3 muscles surrounding the shoulder joint during the performance of a chest press exercise at several angles. J Strength Cond Res. 2010 Jul;24(7):1925-30.
- Vigotsky AD, Halperin I, Lehman GJ, Trajano GS, Vieira TM. Interpreting Signal Amplitudes in Surface Electromyography Studies in Sport and Rehabilitation Sciences. Front Physiol. 2018 Jan 4;8:985.
- Vigotsky AD, Halperin I, Trajano GS, Vieira TM. Longing for a Longitudinal Proxy: Acutely Measured Surface EMG Amplitude is not a Validated Predictor of Muscle Hypertrophy. Sports Med. 2022 Feb;52(2):193-199.
- Haley CA, Zacchilli MA. Pectoralis major injuries: evaluation and treatment. Clin Sports Med. 2014 Oct;33(4):739-56.
- Franchi MV, Longo S, Mallinson J, Quinlan JI, Taylor T, Greenhaff PL, et al. Muscle thickness correlates to muscle cross-sectional area in the assessment of strength training-induced hypertrophy. Scand J Med Sci Sports. 2018 Mar;28(3):846-853.


