

Note: This article was the MASS Research Review cover story for February 2024 and is a review of a recent paper by Marcus et al. If you want more content like this, subscribe to MASS.
Key Points
- The present study examined the effects of acute caffeine consumption on cardiac arrhythmias, daily step counts, and sleep outcomes in 100 healthy adults.
- Participants took more steps on coffee days (10,646 steps) than caffeine avoidance days (9665 steps). However, caffeine also led to less sleep (36 fewer minutes per night) and more daily premature ventricular contractions (p < 0.05).
- Caffeine isn’t inherently bad or unhealthy, but we still don’t fully understand its long-term impact on training adaptations and there are plenty of people who are better off without it. If you’re experiencing issues that could potentially be related to caffeine (e.g., headaches, poor sleep, anxiousness, etc.), experimenting with caffeine avoidance might be worthwhile.
Caffeine is one of the few fitness-related topics where the passion of fitness enthusiasts is matched, if not exceeded, by the general public. The interest from lifters is understandable, as meta-analyses indicate that caffeine can acutely enhance a variety of performance outcomes including strength and power (as covered in this MASS video). Interest from non-lifters is equally understandable, as everyone could use a morning boost of energy and caffeinated beverages like tea and coffee play a prominent role in many cultures. Approximately 85% of American adults consume a caffeinated beverage daily (2), and some estimates place their average daily caffeine intake just north of 200 mg/day (3). That might sound like a lot, but average daily caffeine intakes in Sweden and Finland exceed 400 mg/day (3). To date, one of the top highlights of my career has been presenting at an incredible exercise science conference in Finland – having been there during a relatively cold month, I can vouch for the 400+ mg/day estimate. Coffee was virtually always within reach, and as a coffee lover, I was in heaven.
Having said that, many governments advise citizens to limit their daily caffeine intake to no more than 300-400 mg/day, while some caution that daily intakes above 200 mg/day might lead to unwanted side effects like nervousness or anxiety (4). Caffeinated beverages are also in the news after two recent lawsuits attributed fatal cardiac arrhythmias to the consumption of a particular product at an American restaurant chain. I wouldn’t dare get between a coffee drinker and their morning dose of caffeine, but we shouldn’t turn a blind eye to caffeine’s potential drawbacks just because we enjoy its most desirable characteristics. Instead, we should consult the evidence to determine if the pros outweigh the cons, and that’s exactly what this article intends to do. Marcus et al (1) recently examined the effects of acute caffeine consumption on cardiac arrhythmias, daily step counts, and sleep outcomes, so let’s dive in and see what they found.
Purpose and Hypotheses
Purpose
The purpose of the presently reviewed study was “to examine the effects of caffeinated coffee on cardiac ectopy and arrhythmias, daily step counts, sleep minutes, and serum glucose levels.”
Hypotheses
The researchers did not explicitly state a hypothesis.
Subjects and Methods
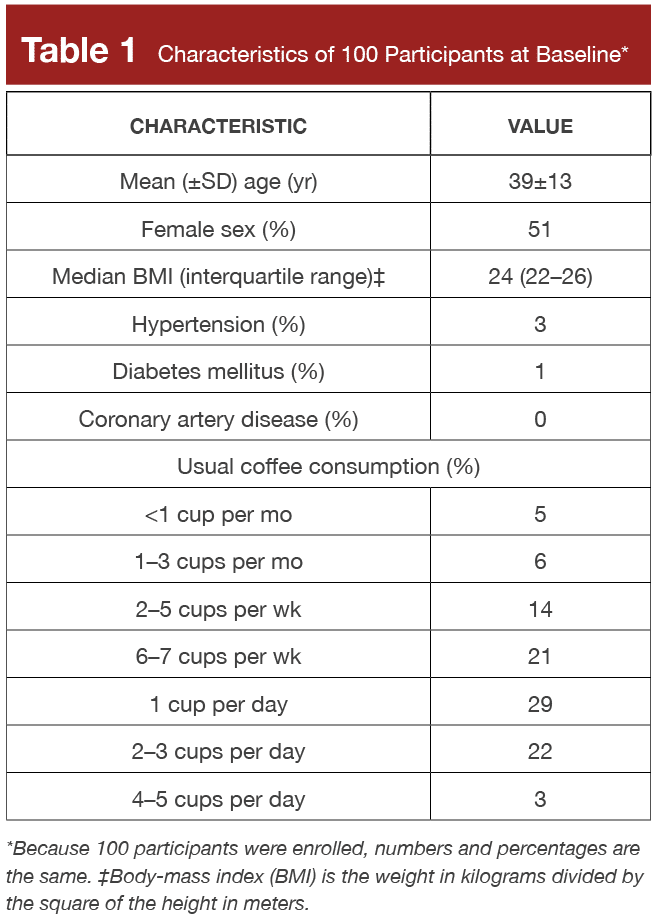
The present study screened 113 potential participants and ended up enrolling 100 eligible adults who consumed caffeinated coffee at least once per year. The researchers excluded participants who had certain heart conditions, took certain medications impacting heart rhythms, or had a medical reason to avoid coffee. The study was a randomized crossover trial; participants were instructed to consume caffeinated coffee or avoid caffeine in a series of seven 2-day sequences (on-off or off-on), with the trial lasting 14 days in total. Each morning, participants received a text message informing them of their assigned condition (caffeinated coffee or no caffeine). These assignments were sent in a randomized order with two-day sequences to ensure that participants would never go more than two consecutive days with caffeine or more than two consecutive days without caffeine.
The primary study outcome was premature atrial contractions, but other outcomes of interest included premature ventricular contractions, arrhythmias, step count, sleep minutes, and glucose levels. To measure these outcomes, participants were fitted with an electrocardiogram (ECG/EKG) patch, activity tracker (Fitbit), and continuous glucose monitor. The researchers took several steps to confirm protocol adherence; participants pressed a button on their ECG patch when they consumed caffeinated coffee, in addition to completing surveys, providing receipts, and downloading a geolocation app to confirm their presence in coffee shops. Participant characteristics are presented in Table 1.
Findings
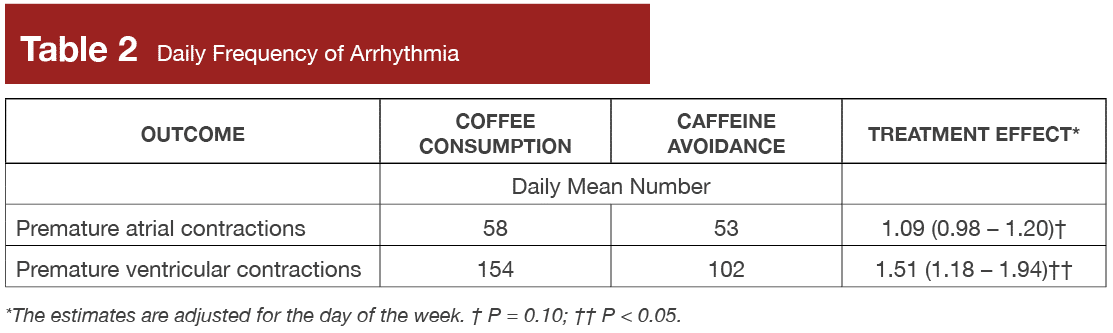
Participants had more premature atrial and ventricular contractions during coffee days than caffeine avoidance days. This was statistically significant for premature ventricular contractions (p < 0.05), but not for premature atrial contractions (p = 0.10). These outcomes are presented in Table 2.
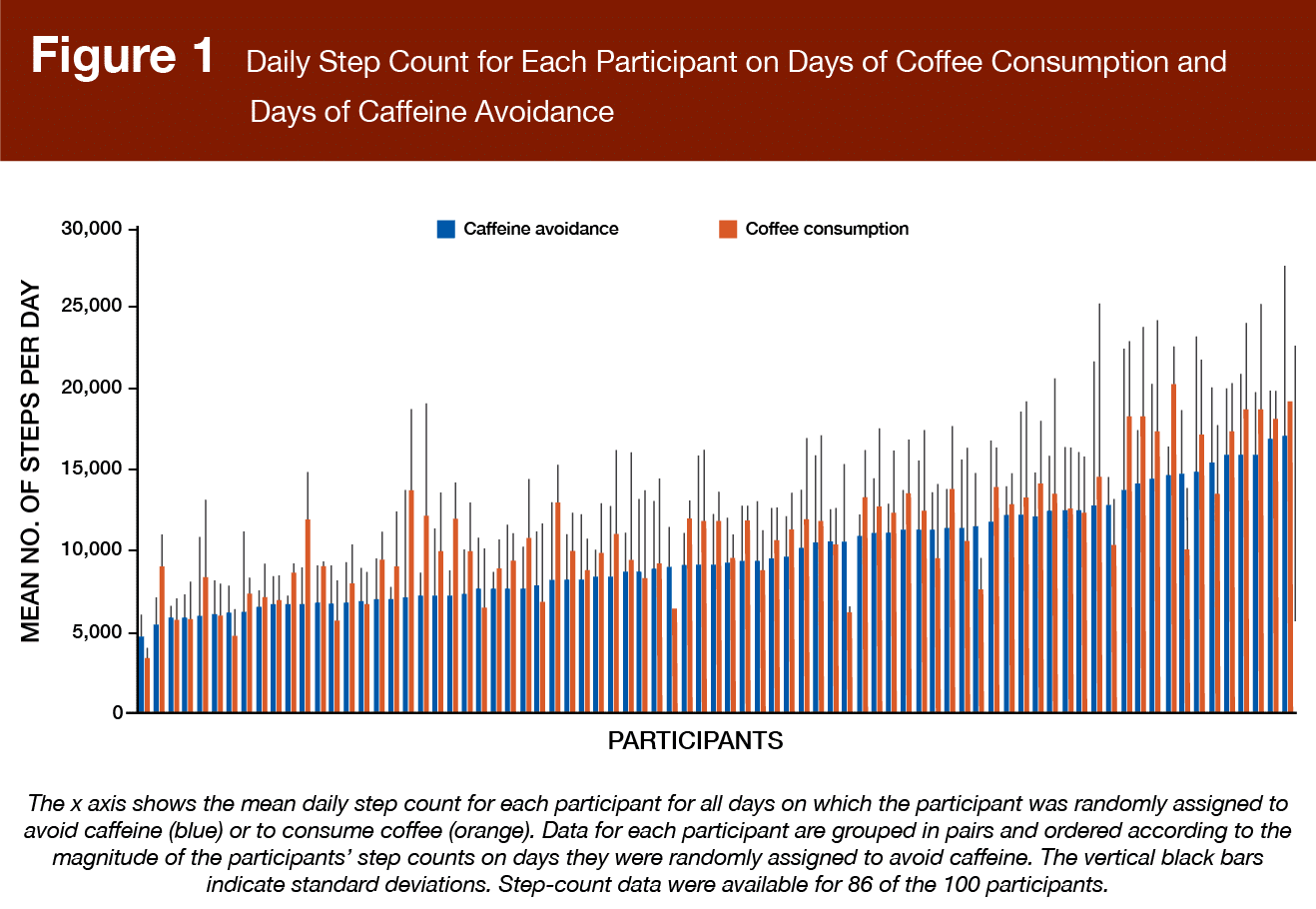
Participants took an average of 1058 additional steps on coffee days in comparison to caffeine avoidance days. This difference was statistically significant (p < 0.05), with a 95% confidence interval ranging from 441 to 1675. These data are presented in Figure 1.
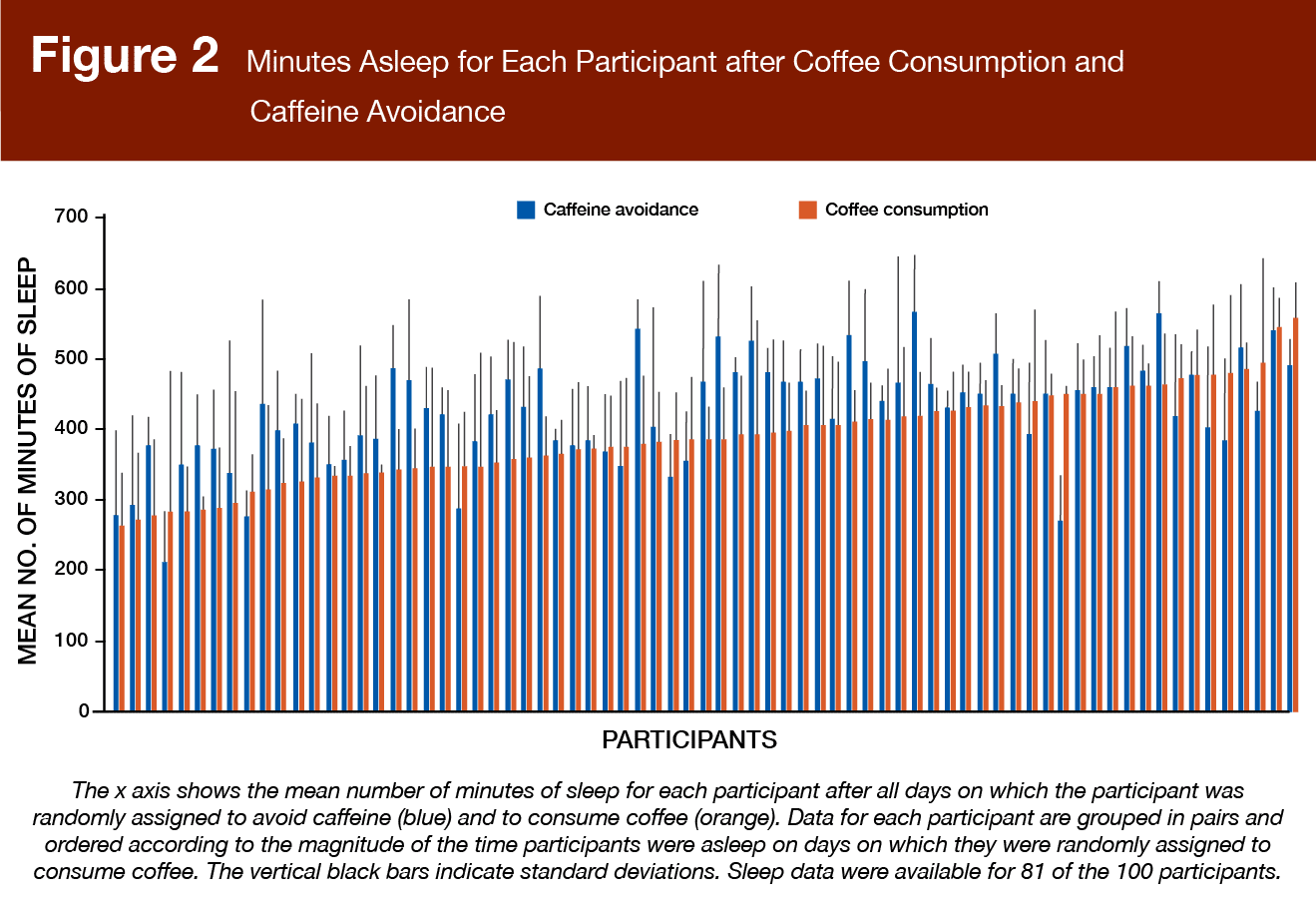
Participants got less sleep on coffee days (for a total of 397 minutes per night) than on caffeine avoidance days (for a total of 432 minutes per night). This mean difference of ~36 minutes was statistically significant (p < 0.05), with a 95% confidence interval ranging from 25 to 47 minutes. These data are presented in Figure 2.
Average blood glucose levels were not meaningfully impacted by coffee or caffeine avoidance. Average glucose levels were 95 mg/dL on coffee days and 96 mg/dL on caffeine avoidance days (mean difference = -0.41 mg/dL; 95% CI, -5.42 to 4.60 mg/dL). In past MASS articles (one, two), we’ve talked about how certain genotypes are associated with faster caffeine metabolism, while other genotypes are associated with slower caffeine metabolism. In the present study, these genotypes did not have a consistent impact on outcomes. Participants with faster genotypes tended to have more premature ventricular contractions on coffee days, whereas participants with slower genotypes tended to experience larger sleep reductions on coffee days. In other words, there was a tendency for fast metabolizers to have better sleep-related outcomes, but worse heart-related outcomes. Genotype had virtually no impact on step count responses to caffeine.
Interpretation
We’ve presented the case “for” caffeine on many occasions within the pages of MASS, and it’s an easy case to make. First and foremost, people love caffeine and the beverages that carry it. Across numerous countries, the vast majority of adults consume caffeinated beverages on a regular basis because they love the beverage itself or enjoy a quick energy boost. In addition, meta-analyses indicate that acute caffeine consumption improves a variety of exercise-related outcomes including endurance, strength, and power (5). On top of all that, the presently reviewed study suggests that caffeine consumption can boost the amount of physical activity you accrue throughout the day, which is generally favorable for health-related outcomes. Nonetheless, against my better judgment, my goal in this article is to present the case “against” caffeine.
Many lifters and athletes refuse to entertain the idea of ditching caffeine because they are hesitant to forego the ergogenic (performance-enhancing) effect of caffeine consumption. While that perspective is understandable, there are valid reasons to challenge (or at least question) the premise. First and foremost, it’s important to recognize that caffeine’s effects on strength and power outcomes tend to be modest in magnitude, with meta-analyses reporting Cohen’s d effect sizes in the 0.1 to 0.3 range (5). That’s a respectable effect size for a dietary supplement (given that so few of them actually work), but it’s certainly not going to make a game-changing impact in the long run. Speaking of the long run, I’ve noted in a previous MASS article that cross-sectional caffeine supplementation studies report acute performance improvements in habitual caffeine users (6). However, there are very few longitudinal studies that actually quantify caffeine’s performance-enhancing effects over an extended timeline of repeated use. One such study (7) was previously reviewed in MASS, and the results hinted at reduced effect sizes over the course of 20 days. There’s also a glaring lack of studies exploring the effects of caffeine withdrawal on exercise performance. So, despite cross-sectional studies reporting acute performance enhancement when habitual caffeine users consume pre-exercise caffeine (6), it’s often difficult to determine if caffeine is merely overcoming performance impairments induced by caffeine withdrawal symptoms. In such a scenario, caffeine would be restoring typical performance levels rather than elevating performance beyond an individual’s typical level. Based on the lack of direct evidence related to these considerations, it’s hard to definitively conclude that routinely supplementing with caffeine before exercise will meaningfully boost performance in the long run.
On a related note, there are very few studies exploring chronic training adaptations in response to habitual pre-exercise caffeine supplementation. People often assume that caffeine must facilitate better training adaptations over time because it acutely enhances performance. While it’s intuitive to assume that acutely enhancing training performance will inevitably lead to better training adaptations over time, that’s not always the case. Some folks draw conclusions about chronic caffeine consumption based on multi-ingredient pre-workout supplement studies, but this is a risky extrapolation to make. Pre-workout supplements typically contain caffeine in conjunction with several other ergogenic ingredients, which makes it difficult to discern the effects attributable to caffeine itself. We previously reviewed a study (8) that directly investigated the effects of regular caffeine supplementation on chronic training adaptations. While the results leaned very slightly in favor of the caffeine group (compared to the placebo group), the findings were not statistically significant. In summary, we still don’t know if chronic pre-exercise caffeine supplementation actually improves training adaptations for lifters.
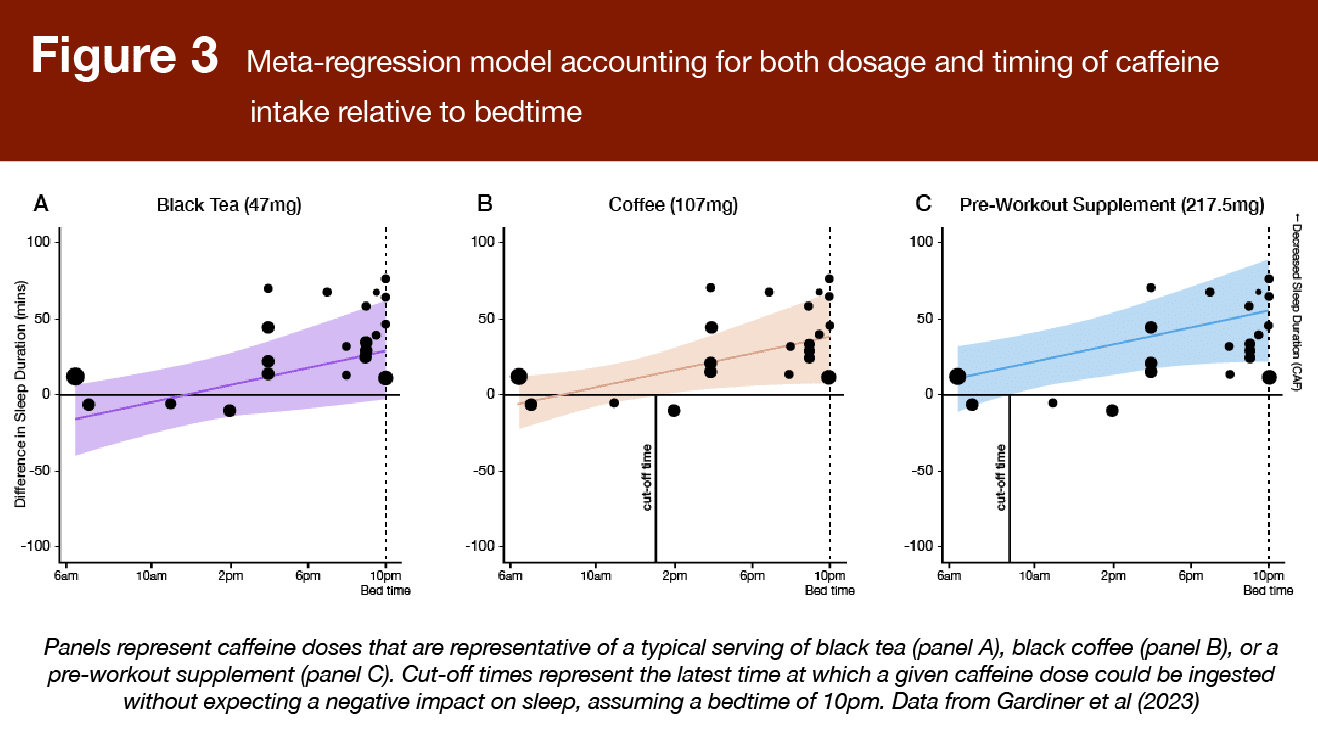
While habituation is an important consideration for chronic caffeine use, sleep impairment is as well. Back in 2013, a study by Drake and colleagues (9) sought to determine how the timing of caffeine consumption impacts sleep quality. Participants either consumed no caffeine or consumed 400mg of caffeine 0, 3, and 6 hours prior to bed. Results indicated that caffeine impaired sleep quality at all time points measured. While this is often misinterpreted as suggesting that you should stop consuming caffeine 6 hours before bed, the results actually don’t help us determine when the “ideal” cut-off time would be. Knowing that caffeine impairs sleep 6 hours before bed doesn’t give us any evidence indicating that sleep is not impaired when caffeine is consumed 7 hours before bed. As reviewed in a previous issue of MASS, a recent meta-regression (10) provides much more practical guidance regarding caffeine timing. As you might expect, Gardiner and colleagues found that caffeine dose impacted caffeine timing with regards to sleep disruption. They concluded that you’d want to consume a 217.5mg dose at least 13 hours before bed and a 107mg dose at least 9 hours before bed, whereas smaller doses (<50mg) don’t seem to meaningfully impact sleep quality. These findings are summarized in Figure 3. I believe it’s safe to assume that these doses should be viewed as cumulative in nature; if you have 100mg at 9 a.m. and 100mg at 1 p.m., the “dose” at 1 p.m. would be greater than 100mg but lower than 200mg, as only a small portion of the 11 a.m. dose would be metabolized and cleared from the bloodstream by 1 p.m.
The presently reviewed study found positive effects on step counts, but it broadly reinforces concerns about caffeine intake and sleep quality impairment. Caffeine lovers often downplay these concerns by leaning on one of two justifications: habituation or genotype. If you dig into the supplementary materials of the present study, you’ll find partial support for these justifications. For example, some people suggest that they’re so habituated to caffeine’s wakefulness effects that late-night caffeine intake fails to impact their sleep. In the present study, people who regularly consumed 1 or more cups of coffee per day at baseline experienced an average sleep reduction of -28.9 minutes on caffeine days, whereas people who regularly consumed less than one cup per day experienced an average sleep reduction of -52.6 minutes. This may indirectly suggest that daily caffeine consumption attenuates, but doesn’t eliminate, negative impacts on sleep. In addition, some people suggest that they’re “immune” to caffeine’s effects on sleep because they’ve got the genotype associated with faster caffeine metabolism. In the present study, individuals with intermediate and slow caffeine genotypes lost an average of 34 and 47 minutes of sleep per night (respectively) on caffeine days, whereas fast metabolizers experienced a mean increase of 33 minutes per night. Nonetheless, I’m hesitant to conclude that the typical person can assume (hope) they’re a fast metabolizer and consume late-night caffeine without sleep-related consequences for two reasons. First, we have insufficient information about how much caffeine these individuals consumed and what time of day they consumed it. Second, there were only 13 participants with “fast” genotypes. This increases the likelihood of a spurious finding, and also suggests that the vast majority of participants in this study (who are, in theory, representative of the population they were sampled from) experienced worse sleep on caffeine days.
When it comes to the heart-related outcomes reported in this study, I want to contextualize those a bit. I know my goal in this article was to present a viable case against caffeine, but I don’t want to present a hyperbolic or alarmist argument. If you’ve ever watched a TV show or movie with a hospital scene, you’ve probably seen someone hooked up to a heart monitor, also known as an EKG (elektrokardiogramm) or ECG (electrocardiogram). The classic squiggly pattern reflects the electrical activity of the heart, which dictates the coordinated rhythm and contraction of each heartbeat. The Q wave represents depolarization of the atrium, the QRS wave complex represents the depolarization of the ventricle, and the T wave represents ventricular repolarization (you can learn more about ECGs and heart rhythms here). When we talk about heart arrhythmias, we’re talking about a disruption in the typical rhythm of the heart. In many cases, arrhythmias are transient and benign (this study observed over 100 premature ventricular contractions per day, on average), but they can sometimes lead to potentially life-threatening medical emergencies.
If you follow the news consistently, you sometimes come across surprising stories indicating that someone died from a high, but not astronomically high, dose of caffeine (for example, 400-800 mg or so). Mounting evidence suggests that individuals with a heart condition called “long QT syndrome” are particularly susceptible to dangerous arrhythmias in response to caffeine consumption (11). Long QT syndrome is exactly what it sounds like – individuals with this condition have a longer-than-average QT interval, which is the length of time between their Q wave and T wave. Caffeine may prolong QT intervals, which can be dangerous for people who have long QT intervals to start with (12). All of that is to say, unless we’re talking about an accidental overdose from a misidentified powder or a completely reckless attempt to intentionally over-consume caffeine, caffeine is unlikely to induce clinically relevant or severe heart arrhythmias in otherwise healthy individuals. However, people with pre-existing heart conditions should consult with a qualified clinician to determine a safe intake range for them.
To conclude this article, I want to share a brief anecdote. I have been a high-dose (≥400-500 mg per day) caffeine consumer for many years, and I recently stopped consuming caffeine entirely. I was too sick to comfortably drink beverages for a few days, so I figured I’d do a little experiment if I was going to experience caffeine withdrawal either way. I’ve been off of caffeine for about a month now, and my observations have been quite interesting. As someone who is generally prone to anxiousness, I’ve noticed a dramatic reduction in anxiety-related symptoms. I used to get headaches if I consumed too little caffeine, but I also got headaches if I consumed too much caffeine. Needless to say, that’s not a problem anymore. I also observed that I feel the need to nap more – on the surface that seems too obvious to be insightful, but I’ve come to realize that I had been undersleeping to a much greater degree than I realized, and caffeine was covering that up like a Band-Aid.
In terms of lifting performance, I haven’t noticed anything at all. At first it felt strange to lift weights without a pre-exercise dose of caffeine, but I’ve come to realize that this was more related to the ritual and subjective experience of caffeination than anything else. I consume caffeine before workouts because it’s what I’ve always done (for many, many years). As a result, I’ve subconsciously associated the subjective feeling of “peak caffeination” as the feeling of being prepared to lift. This psychological link has historically led me to feel unprepared to lift when I’m not caffeinated, but pushing through uncaffeinated workouts has opened my eyes to the fact that caffeine wasn’t doing too much for my workouts in the first place.
We’ve reinforced the importance of sleep many times in previous MASS issues, with research collectively indicating that adequate sleep can be important for performance, body composition, appetite regulation, subjective wellness (generally feeling good), and a variety of other outcomes. We’ve also mentioned the concept of expectancy effects (one, two), like when we expect a placebo to have positive effects or expect a nocebo to have negative effects. In my time away from caffeine, I’ve come to find that caffeine’s net impact on my fitness progress was probably neutral at best – the potential benefits, which may be susceptible to some degree of habituation, came with the drawback of inadequate sleep quality. I’ve also observed that many of the benefits I previously associated with caffeine were most likely influenced by my expectations; I tended to overestimate caffeine’s positive effects and exaggerate the hypothetical downsides of not consuming caffeine. Much to the dismay of the high-powered marketing machine that dictates my every move, I’m not going to make the flashy claim that ditching caffeine will change your life, or that caffeine abstention is the one weird trick you’re missing out on. However, I would encourage you to ask yourself a few questions:
Do you feel better when you consume caffeine, or does caffeine help you avoid bad feelings (e.g., headaches, drowsiness, etc.) that are caused by caffeine in the first place? Are you actually sleeping well enough, or is caffeine masking the signs of insufficient sleep? Does caffeine meaningfully improve your performance, or have you come to expect poor performance when you’re not caffeinated? Do you have any predispositions (e.g., anxiety, slow caffeine metabolism, sleep issues, heart arrhythmias, or family history of heart conditions) that make you question your current level of caffeine consumption?
Don’t get me wrong – most people consume caffeinated beverages regularly and tolerate them quite well. They feel great, perform well, and experience absolutely no adverse outcomes related to their caffeine consumption. However, for some percentage of the human population, caffeine avoidance might be preferable in comparison to regular caffeine consumption. In other words, caffeine is totally fine for most people, but it’s not for everyone, and it’s not without potential drawbacks. I never imagined I would say this, but I much prefer the decaffeinated life based on how it makes me feel on a day-to-day basis. I feel less anxious, well-rested, and ready to perform (mentally and physically) at all hours of the day, and I never find myself feeling unprepared for a mental, social, or physical task because I haven’t had my coffee yet.
But enough with the anecdotes – let’s wrap this up by summarizing the evidence. In the presently reviewed study, caffeine was associated with some pros and some cons. On the bright side, people were more physically active and accrued more steps per day on caffeine. However, caffeine consumption led to sleep impairment and increased frequency of heart arrhythmias. Caffeine is not inherently bad for you, and most people will experience no meaningful improvements in their health, wellness, or performance if they scale back from two daily cups of coffee to zero. Nonetheless, if you have been diagnosed with a heart condition (or suspect that you might have an undiagnosed heart condition), you should check with a qualified healthcare professional to thoroughly explore the matter and determine an appropriate caffeine intake level for your situation. If you’re experiencing issues that could potentially be related to caffeine (e.g., headaches, poor sleep, anxiousness, etc.), or if you’re simply getting way out of hand with your daily caffeine dosage, it might be time to ask yourself the questions listed in this article to determine if a caffeine-free experiment is a worthwhile pursuit.
Next Steps
Surprisingly enough, we still have a lot to learn about caffeine. I’d like to see more experimental research pertaining to how different caffeine doses and timing strategies impact sleep, and how we can explain different subjective experiences (i.e., some people suggest that caffeine has no impact on their sleep, while others report being highly sensitive to it). I’m particularly interested in finding out if these divergent impacts on subjective sleep quality are related to rate of caffeine metabolism, habituation among regular caffeine consumers, inaccurate self-assessments of sleep quality, or something else entirely. On the fitness side of things, I think we need a few longitudinal studies to examine how caffeine’s effects on strength and power change over time and how caffeine withdrawal impacts exercise performance. These types of studies would be perfect for a master’s-level thesis project or as part of a multi-study doctoral dissertation – they address a straightforward question and could be completed with very modest budgets and relatively short study timelines. Finally, it’d be great to see more longitudinal studies that actually quantify caffeine’s effects on chronic training adaptations rather than acute performance metrics.
Application and Takeaways
Caffeine acutely improves performance and may passively lead to higher physical activity levels. However, caffeine can impair sleep, and its effects on long-term training adaptations are currently uncertain. In addition, caffeine can worsen anxiety symptoms and lead to clinically relevant arrhythmias in people with pre-existing heart conditions. Caffeine isn’t inherently bad, but it’s not for everybody. Caffeine consumption habits should be individualized to fit your goals, preferences, subjective experiences, and medical considerations.
Get more articles like this
This article was the cover story for the February 2024 issue of MASS Research Review. If you’d like to read the full, 93-page publication (and dive into the MASS archives), you can subscribe to MASS here.
Subscribers get a new edition of MASS each month. Each issue includes research review articles, video presentations, and audio summaries. PDF issues are usually around 100 pages long.
References
- Marcus GM, Rosenthal DG, Nah G, Vittinghoff E, Fang C, Ogomori K, et al. Acute Effects of Coffee Consumption on Health among Ambulatory Adults. N Engl J Med. 2023 Mar 23;388(12):1092–100.
- Mitchell DC, Knight CA, Hockenberry J, Teplansky R, Hartman TJ. Beverage caffeine intakes in the U.S. Food Chem Toxicol. 2014 Jan;63:136–42.
- Fredholm BB, Bättig K, Holmén J, Nehlig A, Zvartau EE. Actions of caffeine in the brain with special reference to factors that contribute to its widespread use. Pharmacol Rev. 1999 Mar;51(1):83–133.
- Reyes CM, Cornelis MC. Caffeine in the Diet: Country-Level Consumption and Guidelines. Nutrients. 2018 Nov 15;10(11):1772.
- Grgic J, Grgic I, Pickering C, Schoenfeld BJ, Bishop DJ, Pedisic Z. Wake up and smell the coffee: caffeine supplementation and exercise performance-an umbrella review of 21 published meta-analyses. Br J Sports Med. 2020 Jun;54(11):681–8.
- Carvalho A, Marticorena FM, Grecco BH, Barreto G, Saunders B. Can I Have My Coffee and Drink It? A Systematic Review and Meta-analysis to Determine Whether Habitual Caffeine Consumption Affects the Ergogenic Effect of Caffeine. Sports Med. 2022 Sep;52(9):2209–20.
- Lara B, Ruiz-Moreno C, Salinero JJ, Del Coso J. Time course of tolerance to the performance benefits of caffeine. PLoS ONE. 2019 Jan 23;14(1):e0210275.
- Giráldez-Costas V, Ruíz-Moreno C, González-García J, Lara B, Del Coso J, Salinero JJ. Pre-exercise Caffeine Intake Enhances Bench Press Strength Training Adaptations. Front Nutr. 2021 Jan 26:8:622564.
- Drake C, Roehrs T, Shambroom J, Roth T. Caffeine effects on sleep taken 0, 3, or 6 hours before going to bed. J Clin Sleep Med. 2013 Nov 15;9(11):1195–200.
- Gardiner C, Weakley J, Burke LM, Roach GD, Sargent C, Maniar N, et al. The effect of caffeine on subsequent sleep: A systematic review and meta-analysis. Sleep Med Rev. 2023 Feb 6;69:101764.
- Gray B, Ingles J, Medi C, Driscoll T, Semsarian C. Cardiovascular Effects of Energy Drinks in Familial Long QT Syndrome: A Randomized Cross-Over Study. Int J Cardiol. 2017 Mar 15;231:150–4.
- Shah SA, Szeto AH, Farewell R, Shek A, Fan D, Quach KN, et al. Impact of High Volume Energy Drink Consumption on Electrocardiographic and Blood Pressure Parameters: A Randomized Trial. J Am Heart Assoc. 2019 Jun 4;8(11):e011318.


