
This article was first published in MASS Research Review and is a review and breakdown of a recent study. The study reviewed is Effects of Vitamin D3 Supplementation on Serum 25(OH)D Concentration and Strength in Athletes: A Systematic Review and Meta-analysis of Randomized Controlled Trials by Han et al. (2019)
Key Points
- While much of the vitamin D literature focuses on the general population, the current meta-analysis (1) sought to determine if vitamin D supplementation enhances strength performance in athletes
- In order to make the results a bit more intuitive and interpretable, I re-crunched the numbers. Overall, there was a small effect of vitamin D supplements (d = 0.20, p = 0.34). If you divide up the results by performance outcome, the effect size for bench press was -0.12 (p = 0.54), and the effect size for isokinetic leg extension was 0.63 (p = 0.01).
- The largest effects of vitamin D supplementation were observed in the samples who started out with the lowest blood vitamin D levels. While there appears to be a discrepancy between upper body and lower body outcomes, this might be due to the methods used to measure each strength outcome.
It probably shouldn’t be too controversial to suggest that, in general, vitamin deficiencies aren’t a positive thing. However, vitamin D has a special status in the eyes of most lifters, as researchers have previously suggested that vitamin D supplementation could potentially enhance aerobic performance, strength performance, muscle growth, and recovery from exercise (2). Unfortunately, there’s also a bit of uncertainty associated with the management of blood vitamin D levels; there’s an active debate about whether the optimal range is above 50 nmol/L or 75 nmol/L, blood levels are meaningfully influenced by latitude and magnitude of sun exposure (which is difficult to practically quantify), and excessively high blood levels are also problematic. Dr. Helms has previously discussed vitamin D supplementation in two previous MASS articles, but this month, there’s a new vitamin D meta-analysis (1) to report and interpret. Authors of the current paper (1) specifically evaluated the effects of vitamin D supplementation on strength outcomes in athletes. Results indicated that supplementation significantly increased blood vitamin D levels, but effects on bench press strength (effect size [d] = -0.07, p = 0.72) and isokinetic leg extension strength (d = 2.14, p = 0.12) were not statistically significant, nor was the overall effect on both strength outcomes pooled together (d = 0.75, p = 0.17). Having said that, I think these numbers should be taken with a grain of salt. This article explains why I feel that way and discusses whether or not vitamin D is an advisable supplementation strategy.
Purpose and Hypotheses
Purpose
The purpose of this meta-analysis was “to investigate the effects of vitamin D3 supplementation on skeletal muscle strength in athletes.” As an additional outcome, they also analyzed the effects of vitamin D3 supplementation on serum vitamin D levels.
Hypotheses
The authors hypothesized that the meta-analysis would find that vitamin D3 supplementation significantly increases serum vitamin D levels and significantly improves strength performance.
Subjects and Methods
Subjects
As a meta-analysis, this paper pooled the results of multiple studies. A defining characteristic of this meta-analysis was that it only included studies that recruited athletes. The sports represented included taekwondo, soccer, judo, rugby, and football. Strength data were available for a total of 80 athletes, with bench press data for 49 athletes and isokinetic leg extension data for 31 athletes.
Methods
The whole point of a meta-analysis is to search the literature systematically, then mathematically pool the results together to summarize the collective findings. The authors searched the common research databases and only included randomized controlled trials that specifically evaluated strength outcomes in athletes taking oral vitamin D3 supplements. They excluded any potential studies that involved non-athletes, vitamin D2 supplementation, interventions utilizing multivitamins, and studies that included athletes with illnesses or medical conditions that could have potentially altered outcomes of interest.
With meta-analyses, you are working toward calculating a pooled effect size. In order to do that, an effect size (Cohen’s d, or some similar form of standardized mean difference) is calculated for each study included. Typically, for this type of literature, you’d calculate the effect size based on the change in the placebo group (from pre-testing to post-testing), the change in the vitamin D group, and then some form of standard deviation for each group– either the standard deviation of the pre-test or post-test value, or the standard deviation of the change from pre- to post-testing.
For the current meta-analysis, they took a very different approach. Effect sizes were calculated using only the pre-test value in the vitamin D group, the post-test value in the vitamin D group, and the standard deviations at each time point. This is quite atypical, and totally ignores a key, defining feature of these studies, which is that they included a placebo group. The strength of the placebo-controlled design is that we can directly evaluate the effect of the treatment above and beyond the effect of the placebo; to ignore this in the effect size calculation is to adopt a less informative interpretation of each study’s individual results. Off the top of my head, I can only specifically recall seeing one other recent meta-analysis use this approach (3), and it was subsequently retracted, accompanied by a message stating that, “The authors have retracted this article because after publication it was brought to their attention that the statistical approach is not appropriate.” I believe they’re referring to the manner in which the effect sizes were calculated, but unfortunately no details were provided.
Findings
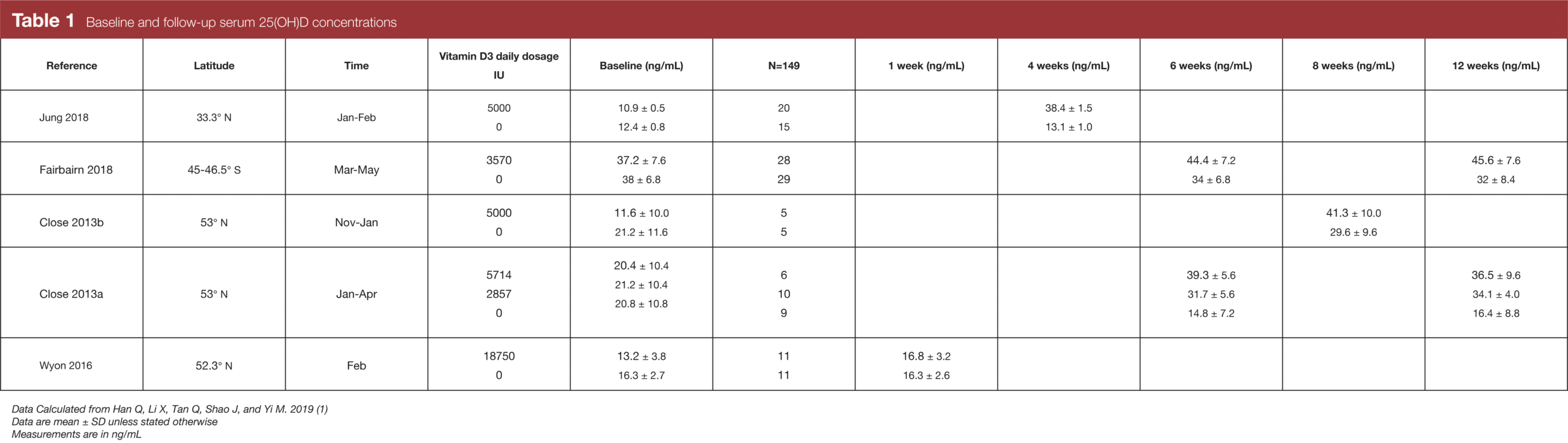
As one would expect, oral vitamin D supplementation significantly increased blood vitamin D levels; the effect size was d = 3.0 for all studies together, and d = 1.18 after removing one study with a fairly high dropout rate. I have used informal language up to this point, so I should clarify that “blood vitamin D levels” refers more specifically to serum levels of 25-hydroxyvitamin D, or 25(OH)D. The liver converts vitamin D3 into 25(OH)D, which is then converted to 1,25-hydroxyvitamin D. While 1,25-hydroxyvitamin D is technically the active form of vitamin D, researchers typically measure 25(OH)D because it has a longer half-life in the blood, and its circulating levels are about 1,000 times higher (4). Table 1 shows the baseline and post-test values for blood vitamin D levels, along with some key study characteristics related to vitamin D levels, such as latitude and time of year. To assist with interpretation, keep in mind that 1 ng/mL is equivalent to 2.5 nmol/L, and some scientists suggest that the ideal blood vitamin D range is 20-40 ng/mL (50-100 nmol/L), whereas others suggest that it’s 30-50 ng/mL (75-125 nmol/L).
If you read my previous review of a fairly recent creatine meta-analysis, you know that I tend to be really picky about how meta-analyses are done. At first glance, it might seem like I’m splitting hairs and making a huge deal out of minor differences. However, the current meta-analysis presents us with an awesome example of why meta-analytic methods matter, big time. There was another vitamin D meta-analysis by Tomlinson et al in 2015 (5), which included some of the same data. Both included a 2013 study by Close et al (6), which evaluated two different vitamin D doses, looking at bench press as an outcome variable. For the same exact data, Tomlinson et al calculated an effect size of d = 0.75 for the low-dose treatment, whereas the current meta-analysis calculated an effect size of d = 0.14. To contextualize that gap of around 0.6, it’s worth noting that caffeine typically improves strength and power outcomes with an effect size of around 0.2-0.3 (7), and a 2003 meta-analysis found that the effect of creatine on 1RM outcomes was around 0.32 (8). Furthermore, the current study computed an effect size of 3.55 for Jung et al (9), while the true value should be less than 1 if you use virtually any commonly accepted method of effect size calculation. So, while I admittedly enjoy exploring these details more than anyone should, it’s safe to say that these things matter.
As I noted in the methods section, the authors of the current meta-analysis took a very unconventional statistical approach. It should also be noted that they got standard deviation and standard error mixed up for Jung et al (9) and omitted the higher-velocity leg extension data from Jung et al (9) and Wyon et al (10) without explanation or justification. Taken together, we have multiple justifiable reasons to disregard the values calculated in the original paper.
With these considerations in mind, I went ahead and re-crunched the numbers in a way that I find to be more informative. I calculated Hedges’ g as my effect size metric, but its interpretation is extremely similar to Cohen’s d, so I’m just going to use “d” as my general effect size symbol throughout this article. To calculate effect sizes, I compared the change (pre to post) in the supplement group to the change (pre to post) in the placebo group. I used the baseline standard deviation for effect size calculations, and I assumed a within-study correlation of 0.8 when aggregating multiple effect sizes from a single sample. With this approach, the overall pooled effect size ends up being 0.20 (p = 0.34), and the forest plot is presented in Figure 1.
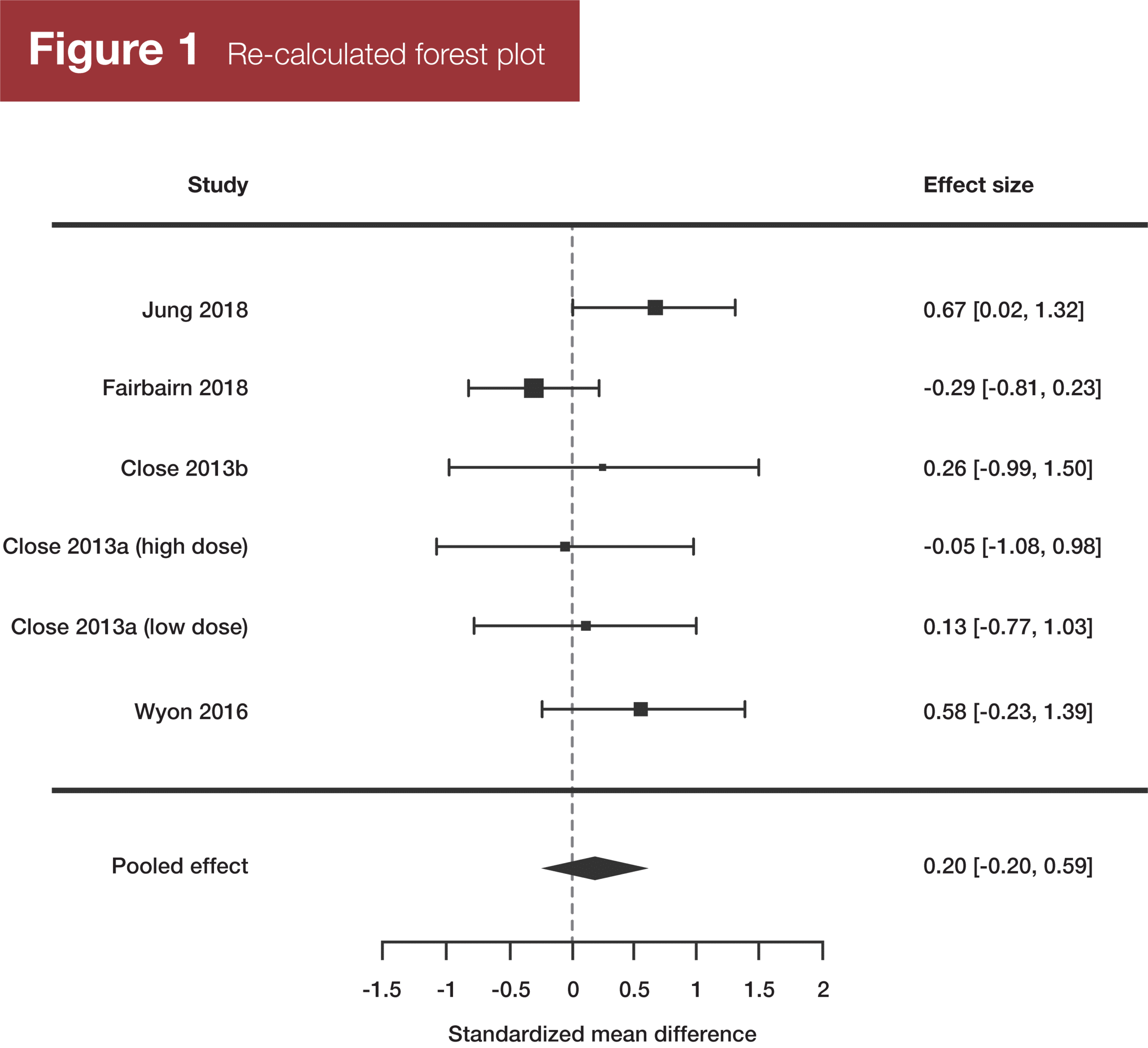
The authors of the current meta-analysis also split the data set to independently look at bench press results and leg extension results. If we do that with the re-calculated values, the effect size for bench press outcomes is -0.12 (p = 0.54), and the effect size for leg extension outcomes is 0.63 (p = 0.01).
Prefer to listen? Check out the audio roundtable
Every article we review in MASS has an accompanying audio roundtable just like this one. All of the MASS reviewers (Greg Nuckols, Eric Trexler, Eric Helms, and Mike Zourdos) get together to discuss the findings and applications in practical, easy-to-understand terms. Subscribe to MASS here.
Interpretation
Vitamin D supplementation has become somewhat popular among lifters, likely because low vitamin D levels tend to be quite common. For example, even among healthy athletes, one recent meta-analysis reported that 56% of subjects sampled had inadequate vitamin D levels, which was operationally defined as blood 25(OH)D levels below 32 ng/mL (80 nmol/L) (11). Other studies have shown up to 57%, and even 62%, of athlete samples to have deficient or insufficient vitamin D levels (12). That’s pretty troubling, as low vitamin D levels have been linked to depression, cognitive decline, poor bone health, and decreased neuromuscular function (2). Specifically, vitamin D levels tend to be lower during the winter months, and in individuals who have minimal direct exposure to sunlight, live at high latitudes, or frequently wear sunblock with a high sun protection factor. It’s frequently said that vitamin D levels are typically lower in individuals with darker skin pigmentation, but Dr. Helms made me aware of some research indicating that it might not be that simple (13). In short, individuals with darker skin pigmentation may have lower levels of total blood 25(OH)D concentrations, despite having similar bone density and similar levels of bioavailable 25(OH)D. This is important, because not all of the 25(OH)D in our blood is bioavailable, and it’s the bioavailable 25(OH)D that’s really driving the positive effects of vitamin D.
As noted by Dahlquist et al (2), there are very plausible reasons to believe that correcting vitamin D deficiency or insufficiency would have a positive impact on performance. For example, multiple studies have found correlations between blood vitamin D levels and aerobic fitness (VO2max), and one study found that vitamin D supplementation increased VO2max (14), possibly by influencing oxygen’s binding affinity with hemoglobin. There is also observational and experimental evidence linking vitamin D to muscle force production, which may be related to an increase in the size and number of type II muscle fibers or enhanced calcium sensitivity of the sarcoplasmic reticulum. Much of this research has been conducted in samples of older adults; such studies typically observe notable deficits in neuromuscular function as a result of vitamin D deficiency, which is robustly restored following vitamin D supplementation (15). Other observational and experimental studies have linked vitamin D to higher testosterone levels, reduced post-exercise inflammation, and more rapid recovery from intense exercise (2). In summary, there is reason to believe that vitamin D may positively impact a variety of exercise performance outcomes due to its effects on sarcoplasmic reticula, testosterone, hypertrophy, recovery, and even oxygen delivery.
When I first saw the results of the current meta-analysis, I was pretty skeptical. The effect sizes just seemed way too large and inconsistent, and further digging verified that some additional number-crunching was warranted. After re-running the analysis, this literature is much more in line with what I would have expected. The overall effect size is a very realistic d = 0.20, and the overall analysis was not statistically significant. However, if we look a little bit closer at the results, a couple of interesting patterns appear.
The first pattern is pretty intuitive: The studies with the three largest effect sizes were the studies reporting the lowest baseline vitamin D levels in the supplement group. In each of these studies, the baseline value for the supplement group was under 14 ng/mL, while the other three studies had baseline values above 20 ng/mL. By far, the least impressive results were reported by Fairbairn et al (16), with an effect size of -0.29. Their supplement group had the highest baseline vitamin D levels by far, with an initial value of over 37 ng/mL. To contextualize that, no other group receiving supplements in this meta-analysis had a baseline value over 21.2 ng/mL. In addition, while there is some ongoing debate on exactly what the “ideal” range of blood vitamin D levels is, 37 ng/mL is considered sufficient under every set of recommendations that I’ve come across.
The second pattern is pretty intriguing: The studies within this meta-analysis seem to indicate that vitamin D was beneficial for lower-body exercise, but not upper-body exercise. This was also reported in a recent meta-analysis by Zhang et al (17), but a 2015 meta-analysis by Tomlinson et al (5) reported nearly identical effects for a variety of upper-body and lower-body exercises following vitamin D supplementation. Of course, for the current set of data, it’s possible that the explanation is simply that the studies looking at lower-body exercises coincidentally happened to, on average, report lower baseline vitamin D levels. It’s also possible that the observed difference between upper-body and lower-body results may relate to physiological explanations. For example, Zhang et al (17) speculated that lower-body musculature could be more responsive to vitamin D supplementation due to greater vitamin D receptor density in those particular muscle groups, or due to physiological differences related to the fact that the lower-body musculature is much more heavily involved in activities of daily living. Despite these possibilities, I have a hunch that this apparent difference could be explained by research methods.
In the current study, upper-body strength was exclusively defined as bench press strength, whereas lower-body strength was defined as isokinetic leg extension. Isokinetic leg extension doesn’t really mimic the way we train in the gym or compete on the platform, but it’s awesome for research purposes. You can control the speed of contraction, the range of motion, and every joint angle imaginable, for a measurement that can be reliably replicated at multiple visits. In addition, you’re taking a sensitive, granular torque measurement, down to the exact Newton meter. With bench press, things are different. Setups can vary from day to day. Participants know the load on the bar, have some degree of an emotional connection to it, and deep down, they probably want their post-test value to be higher than their pre-test value, despite not knowing what treatment group they’re in. It’s much more difficult to standardize the movement and to ensure that you’re getting a perfectly equivalent, maximal effort at all visits. In addition, how much can we realistically expect an athlete’s (note: typically well-trained, but not hyper-focused on bench pressing) bench press to increase from vitamin D supplementation over the span of a fairly short-term study? Many labs lack fractional plates, so for a number of subjects, testing probably approximated a categorical variable: they could either add another 1.25kg plate to each side, or maybe two, or maybe none.
Perhaps the strongest evidence supporting this theory is presented by Tomlinson et al (5). They looked at a variety of upper body and lower body outcomes following vitamin D supplementation, using a broader selection of studies than the current meta-analysis. The pooled effect sizes for upper body results and lower body results were virtually identical. However, both the upper body and lower body categories included exercise tests that used gym machines, free weights, and dynamometers (handgrip or isokinetic). For the upper body outcomes (eight total), the two lowest effect sizes were from tests using gym machines or free weights, with the six highest effect sizes coming from dynamometry. For the lower body outcomes (eight total), the three lowest effect sizes were from tests using gym machines or free weights, with the five highest effect sizes coming from dynamometry. Further, a 2013 study (18) sought to determine if blood vitamin D levels correlated with upper body or lower body strength measurements in a sample of 419 men and women aged 20-76 years. Notably, all measurements were taken via dynamometry. When controlling for age and sex, blood vitamin D level was significantly associated with both arm and leg strength. If anything, the relationship was more consistent for upper-body strength than lower-body strength after controlling for additional covariates.
The studies included in this meta-analysis suggest that vitamin D supplementation can have a small but positive effect on strength outcomes, particularly if supplementation is bringing you from deficient or insufficient vitamin D levels to sufficient vitamin D status. While it’s true that effects appear to be more pronounced in lower body exercise than upper body, I’m inclined to believe that this is an artifact of the measurement techniques used rather than a “real” physiological difference. As I noted previously, there’s a bit of a debate regarding what “sufficient” really is; some people suggest that blood levels of 25(OH)D should be above 20 ng/mL (50 nmol/L), while other suggest it should be above 30 ng/mL (75 nmol/L). However, as with most things in physiology, more is not always better. Vitamin D enhances calcium absorption from the gut, in addition to increasing mineralization and bone resorption (that is, the process by which bone tissue is broken down and its minerals are released into the blood) by stimulating bone cells to produce receptor activator nuclear factor-kB ligand. As a result, chronically high vitamin D levels could potentially lead to excessive blood calcium levels, which could increase the risk of kidney stones or cardiovascular issues related to vascular calcification (2). To be fair, serum 25(OH)D concentrations below 140 don’t seem to be associated with high blood calcium levels, and acutely observable adverse effects typically aren’t reported until blood 25(OH)D levels get up around 200 nmol/L, which would probably require a daily vitamin D dose of around 40,000 IU per day (2). Nonetheless, the take-home point remains the same: You don’t want your vitamin D levels to be too low or too high. Finally, individuals with a relatively high degree of skin pigmentation might want to rely on metrics other than total blood 25(OH)D levels to determine if they should consider supplementation. In my opinion, the best approach to managing your vitamin D levels with confidence is to get some valid blood testing done, and put a supplementation plan together with your doctor or otherwise qualified healthcare practitioner.
Next Steps
For lifters, it looks like there are two key questions to be answered in the near future. When it comes to blood vitamin D levels, there still isn’t a consensus about how much is enough. So, it’d be great to more conclusively identify the optimal range of blood vitamin D levels in which neuromuscular performance is optimized. In addition, I’d like to see some follow-up work investigating the apparently differential responses between upper-body and lower-body musculature. Ideally, we’d see studies that involve both upper-body and lower-body measurements within the same subjects, using both free weights and dynamometry, to figure out if the observed difference in the current meta-analysis is attributable to physiology or measurement precision. For the free weight measurements, it’d be great if researchers blind the loads being used and utilize fractional plates, which would serve to minimize confounding effects from psychological factors and enhance the precision of 1RM estimates.
Application and Takeaways
Maintaining sufficient blood vitamin D levels definitely seems like a good idea, both for health and performance. The studies within this meta-analysis suggest that vitamin D supplementation can have a small but meaningful effect on strength performance, but only if supplementation is bringing your suboptimal baseline vitamin D levels up into the optimal range. There is some evidence suggesting that effects are more pronounced in lower-body strength tasks than upper-body tasks, but I suspect this is more of a methods issue than a physiology issue. Finally, it’s important to remember that more vitamin D isn’t always better. If you suspect that your vitamin D is low, the best approach is to get your blood tested and work with a qualified healthcare professional to get a supplementation plan together.
References
- Han Q, Li X, Tan Q, Shao J, Yi M. Effects of vitamin D3 supplementation on serum 25(OH)D concentration and strength in athletes: a systematic review and meta-analysis of randomized controlled trials. J Int Soc Sports Nutr. 2019 Nov 26;16(1):55.
- Dahlquist DT, Dieter BP, Koehle MS. Plausible ergogenic effects of vitamin D on athletic performance and recovery. J Int Soc Sports Nutr. 2015;12:33.
- Siddique U, Rahman S, Frazer AK, Howatson G, Kidgell DJ. RETRACTED ARTICLE: Determining the Sites of Neural Adaptations to Resistance Training: A Systematic Review and Meta-Analysis. Sports Med. 2019 Nov;49(11):1809.
- Lukaszuk JM, Luebbers PE. 25(OH)D status: Effect of D3 supplement. Obes Sci Pract. 2017 Mar;3(1):99–105.
- Tomlinson PB, Joseph C, Angioi M. Effects of vitamin D supplementation on upper and lower body muscle strength levels in healthy individuals. A systematic review with meta-analysis. J Sci Med Sport. 2015 Sep;18(5):575–80.
- Close GL, Leckey J, Patterson M, Bradley W, Owens DJ, Fraser WD, et al. The effects of vitamin D(3) supplementation on serum total 25[OH]D concentration and physical performance: a randomised dose-response study. Br J Sports Med. 2013 Jul;47(11):692–6.
- Grgic J, Grgic I, Pickering C, Schoenfeld BJ, Bishop DJ, Pedisic Z. Wake up and smell the coffee: caffeine supplementation and exercise performance-an umbrella review of 21 published meta-analyses. Br J Sports Med. 2019, ePub ahead of print.
- Branch JD. Effect of creatine supplementation on body composition and performance: a meta-analysis. Int J Sport Nutr Exerc Metab. 2003 Jun;13(2):198–226.
- Jung HC, Seo MW, Lee S, Jung SW, Song JK. Correcting Vitamin D Insufficiency Improves Some But Not All Aspects of Physical Performance During Winter Training in Taekwondo Athletes. Int J Sport Nutr Exerc Metab. 2018 Nov 1;28(6):635–43.
- Wyon MA, Wolman R, Nevill AM, Cloak R, Metsios GS, Gould D, et al. Acute Effects of Vitamin D3 Supplementation on Muscle Strength in Judoka Athletes: A Randomized Placebo-Controlled, Double-Blind Trial. Clin J Sport Med. 2016 Jul;26(4):279–84.
- Farrokhyar F, Tabasinejad R, Dao D, Peterson D, Ayeni OR, Hadioonzadeh R, et al. Prevalence of vitamin D inadequacy in athletes: a systematic-review and meta-analysis. Sports Med. 2015 Mar;45(3):365–78.
- Ogan D, Pritchett K. Vitamin D and the Athlete: Risks, Recommendations, and Benefits. Nutrients. 2013 May 28;5(6):1856–68.
- Owens DJ, Allison R, Close GL. Vitamin D and the Athlete: Current Perspectives and New Challenges. Sports Med. 2018;48(Suppl 1):3–16.
- Jastrzębski Z. Effect of vitamin D supplementation on the level of physical fitness and blood parameters of rowers during the 8-week high intensity training. Facicula Educ Fiz Şi Sport. 2014;2:57–67.
- Hamilton B. Vitamin D and Human Skeletal Muscle. Scand J Med Sci Sports. 2010 Apr;20(2):182–90.
- Fairbairn KA, Ceelen IJM, Skeaff CM, Cameron CM, Perry TL. Vitamin D3 Supplementation Does Not Improve Sprint Performance in Professional Rugby Players: A Randomized, Placebo-Controlled, Double-Blind Intervention Study. Int J Sport Nutr Exerc Metab. 2018 Jan 1;28(1):1–9.
- Zhang L, Quan M, Cao Z-B. Effect of vitamin D supplementation on upper and lower limb muscle strength and muscle power in athletes: A meta-analysis. PloS One. 2019;14(4):e0215826.
- Grimaldi AS, Parker BA, Capizzi JA, Clarkson PM, Pescatello LS, White MC, et al. 25(OH) vitamin D is associated with greater muscle strength in healthy men and women. Med Sci Sports Exerc. 2013 Jan;45(1):157–62.


